While computed tomography (CT) scans account for only around 10% of imaging exams, they account for 60% of radiation dosage. And when radiologists are seeking to lower radiation dose, CT is a modality that would seem ripe for interventions to reduce variability that is seen across patients, institutions and countries, as evidence suggest that CT doses can be reduced by 50% or more without affecting diagnostic accuracy. .
At this week’s European Congress of Radiology in Vienna, Rebecca Smith-Bindman, MD, Professor in Residence of Radiology, Epidemiology and Biostatistics, Obstetrics, Gynecology and Reproductive Medicine, and Health Policy at the University of California, San Francisco, reported the results of the first international randomized controlled trial (RCT) that compared two interventions for reducing CT dose through audit feedback and sharing best practices.
The trial, CT Dose Collaboratory [NCT 03000751], funded by the U.S. National Institutes of Health and the Patient-Centered Outcomes Research Institute, used a stepped wedge design to compare interventions in each institution:
- A simple audit comparing institutional doses with other institutions in the dose registry combined with provision of tailored recommendations
- A multicomponent intervention that included the audit and tailored recommendations plus an invitation to complete an 8-week educational course on quality improvement and best practices.
The audit information provided was sufficiently granular to be meaningful and included data by individual machine.
Results
CT examinations included: 1,204,939
The proportion of high-dose exams, and the mean effective dose for abdomen, chest, combined chest/abdomen and head CT following each intervention were compared to baseline using hierarchical generalised linear models adjusting for temporal trends.
High-dose CT exams
After the multicomponent intervention, the proportion of high-dose CT exams was reduced 14-38% across the four anatomic areas:
- Abdomen (Odds Ratio [OR] 0.86 [95% CI 0.81, 0.91]
- Chest (OR 0.86 [95% CI 0.81, 0.93])
- Combined abdomen and chest (OR 0.62 [95% CI 0.53, 0.74])
- Head (OR 0.62 [95% CI 0.58, 0.66])
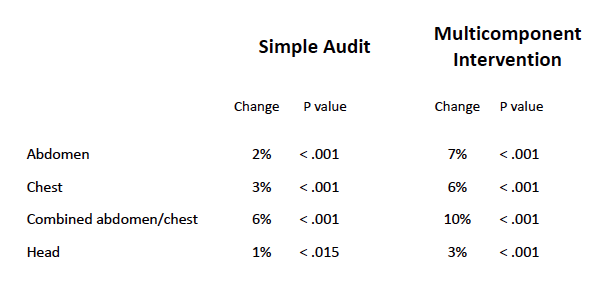
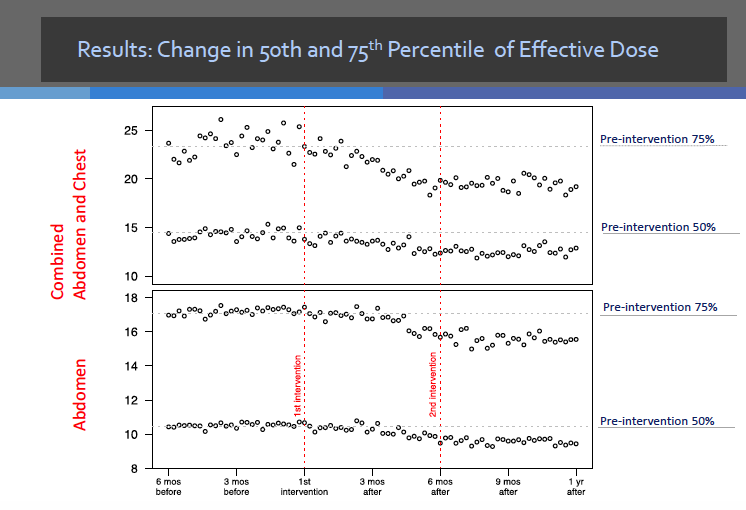
Reduction in mean effective dose
- Abdomen 7%
- Chest 6%
- Combined abdomen and chest 10%
- Head 3%
The simple audit also significantly reduced the proportion of high-dose exams (p<0.05>, and for most anatomic areas, significantly reduced the mean effective dose; however, the magnitudes were smaller than for the multicomponent intervention. Dose reduction was seen across all kinds of equipment, noted Smith-Bindman.
Table 1. Likelihood of a high dose examination following the audit and multicomponent intervention
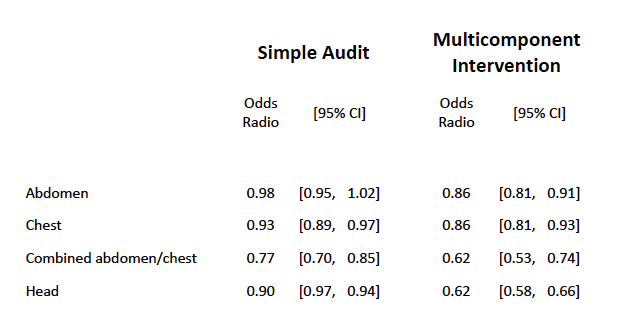
Table 2. Mean effective dose
Next steps
Smith-Bindman explained that they have yet to provide detailed feedback by radiology technologist, but they are looking at how to do this, as they do not want it to be used punitively. She added that they hope that this trial could be a role model for other projects to increase consistency in CT dosage between sites. The learning programme will be made available as virtual online meeting, she added. The research team also intend to create an app to include standards and benchmarks.
The research group also included Philip Chu, MS, Yifei Wang, PhD, Robert Chung, PhD, Andrew J. Einstein, MD, PhD and Diana L. Miglioretti, PhD.
Image credit: Wikimedia Commons
Latest Articles
CT, randomised controlled trial, dose reduction, ECR 2018, #ECR2018
While computed tomography (CT) scans account for only around 10% of imaging exams, they account for 60% of radiation dosage. And when radiologists are see...