The shift to structured radiology reports has increased report clarity for referring providers and is supported by most radiologists. As the movement for increased transparency in healthcare continues, more and more patients are accessing their imaging reports via patient portals.
When radiologists address the clinical question that was posed, avoid the use of abbreviations, and create a report impression that is as simple as possible, we provide real added value via effective communication through our reports. In creating our reports with the patient in mind, and specifically knowing that many patients now directly review their imaging reports, we must be cognisant of the “curse of knowledge.”
The curse of knowledge is a cognitive bias that exists when we assume others have the background to understand our often complex radiology reports. Striving to mitigate the curse of knowledge is important for both patients and referring providers reading our reports, and a report impression that is presented as simply as possible in “lay language” is one tangible step toward this goal. Educating our residents and fellows about these important considerations as they create their reports is imperative to their success as radiologists.
You may also like: Radiologists risks in communicating unexpected findings
INTRODUCTION
The shift to structured reports in radiology is well underway and has been for some time. Reports written in flowing, eloquent prose are becoming less common across all practice settings. Voice recognition software programs have improved considerably over time, and a structured report can provide considerable time savings in many settings. Many practices have created their own standardised report templates, and the RSNA offers a multitude of standardised reports on its website. Reviewing the history of how and why this movement came about is both interesting and educational. Radiology's focus on adding value to the patient's care and healthcare paradigm is also an important and laudable goal. There are various ways to improve report details that could go a long way to providing added value for our patients and referring providers. Lastly, in the era of increasing transparency throughout healthcare, more and more of our patients access their results via patient portals. This is a considerable shift that warrants thought and discussion about how best to serve our patients. It also poses a seismic shift to the radiology report, the product of our work, which was once intended solely for the referring provider. As our target audience changes, so must our reports.
STRUCTURED REPORTS
Looking back at how the shift to structured reports started is fascinating. At a 2007 American College of Radiology Intersociety conference, representatives from various organisations recommended use of structured reports in radiology to improve communication (1). It was also clear that a shift to structured reporting would likely make it easier to extract information from reports, whether for research or quality improvement purposes. As structured reports made their debut in clinical practice, various studies evaluated resulting changes. Schwartz et al. (2) found that both referring providers and radiologists found the content and clarity of structured reports superior to conventional reports. Another study by Bosmans et al. (3) found the majority of referring providers and radiologists preferred receiving itemised reports with clear headings. In addition, Ross et al. (4) showed the use of the word “normal” substantially increased with the shift to structured reporting, indicating a trend toward more definitive reporting. Buckley et al. (5) reported recall for critical diagnoses was 83% for structured reports as compared to 65% for unstructured reports.
ADDING VALUE
The first step to adding value to our patients’ care is creating a high-quality report – the very basis of that is a report free from spelling and voice recognition errors. At first thought this may seem like an easily achievable goal, but as clinical volumes continue to rise and complexity of cases increases, there is often less time for adequate proofreading. Another critical component of a quality report is to ensure the clinical question that was posed to us is addressed. For example, if the question posed is whether there is a bowel obstruction, an appropriate impression for a negative exam might be “No evidence of bowel obstruction, as clinically questioned.”
Avoiding abbreviations is an excellent way to minimise the possibility of miscommunication in your report and to improve report clarity. What seems to you like an abbreviation that “everyone” should know may in fact be unknown to the patient or referrer who reads your report – or it may mean something entirely different to him/her. For example, I work regularly with a very bright medical oncologist in breast tumour boards; he quotes scientific study after scientific study in the most perplexing “oncology alphabet soup” one has ever heard. While he and the one other medical oncologist in the room may be speaking the same “language,” the other sub-specialists (radiologists, pathologists, breast surgeons, radiation oncologists, plastic surgeons) most certainly are not fluent in that particular “language.”
Along the same lines of “languages,” we must remember that terminology and descriptors that are second nature to radiologists are often completely foreign to most providers and patients reading our reports. The danger here is twofold: providers may unknowingly misinterpret terminology; what's more, they (as well as their patients) may be unwilling to request clarification due to a social psychological phenomenon known as “pluralistic ignorance” (6). Specifically, people are unwilling to ask for clarification because they assume everyone else knows the answer – and thereby they assume they should know the answer. For example, if I say a female pelvic MRI shows “an adnexal mass with T1 hyperintense signal precontrast, T2 shading, and no postcontrast enhancement,” any radiologist who reads this exam would say that I am describing an endometrioma. Most anyone else reading this report would not conclude “endometrioma” from that description. In creating our reports, it is important to put the imaging descriptors in the body of the report because they explain how we are arriving at the conclusions we are drawing from this imaging study. However, those descriptors should not be repeated in the impression of our report. The impression should be as “simple” and clear as possible. An appropriate impression for that female pelvic MRI would be “endometrioma.” However, even this succinct impression is unlikely to be easily understood by most patients. The challenges in creating clear reports that are readily understood by both providers and patients are great. A “differential diagnosis,” for example, could be interpreted by the patient as having all those diagnoses. Could there be a role for separate “summary” in radiology reports that is directed exclusively to patients?
When clinical correlation is required for increased diagnostic confidence, it is most helpful to be specific about exactly what you are looking for, rather than offering the generalised and often useless recommendation for “clinical correlation.” For example, if you see an enlarged parathyroid gland on a thyroid ultrasound, suggest correlation with serum calcium. That will be much more useful to your referring provider than “clinical correlation,” which frankly could mean just about anything.
Voice recognition software programs have made it much easier to incorporate data-driven guidelines for imaging follow-up, as these can be embedded in the templates and used when indicated. In our department, we have guidelines for adnexal cysts, lung nodules, thyroid nodules, abdominal aortic aneurysms, to name only a few. Each guideline has a corresponding reference included with it that substantiates our reasons for follow-up recommendations. Your report is more likely to comply with accepted follow-up guidelines if these are built into your reporting system, and your patient's care is more likely to be streamlined if unnecessary follow-up can be avoided. In addition, this allows your referring provider to reference the data upon which the guidelines and recommendations are based if s/he chooses. Lastly, as Dr Hoang (7) has suggested, it may be helpful to both the patient and provider to provide an appropriate context for the findings you are reporting. For example, if an MRI of the spine shows disc desiccation that is expected for the patient's age, stating so may dissuade the referring provider from ordering unnecessary additional imaging and may prevent the patient from worrying about this finding.
While we sometimes take our ability to communicate with others for granted, clear communication is often difficult to achieve successfully. This holds true for radiologists’ ability to communicate with referring providers and patients, perhaps because we assume too much. When we unknowingly assume the audience whom we are communicating with has the education and training to understand what is being conveyed when this may not be the case, we fall victim to a cognitive bias – the “curse of knowledge” (8). As an example of potential miscommunications, consider a survey study comparing radiologists’ and nonradiologists’ interpretations of radiology reports, where there were disagreements on 11/36 terms – some even including “normal” and “diagnostic of” (9)! In an effort to improve reporting clarity, an ever-increasing number of reporting systems modeled on the original BI-RADS (Breast Imaging Reporting and Data System) have been developed. These now span multiple organ systems and include C-RADS (CT colonography), LI-RADS (liver), Lung-RADS, PI-RADS (prostate), TI-RADS (thyroid). These have grown in popularity across different organ systems because of the increased clarity they provide, much like the BI-RADS system when it was introduced many years ago.
PATIENTS AND PORTALS
The movement toward patient access to medical portals started in 2010 with the Open Notes project (10, 11). This effort enrolled 22,000 patients at 3 different clinical sites and provided the first direct way for patients to access their medical information. It was incredibly well received, with 99% wanting continued access to their information, and evidence showing that patients increased understanding of their health and had improved health outcomes (10, 11). In addition, there was little change in the number of telephone inquiries directed to primary care providers which had been an initial concern when the project was launched. Another study from a large healthcare system (12) also showed high satisfaction from both patients and providers when radiology reports were available in the patient portal.
Patient portals are now commonly available across a variety of care settings (Fig. 1), though there are undoubtedly still disparities in level of access based on economic status, internet access, education level, and language barriers. This is a stark contrast to years passed. I still clearly remember an experience as a medical student when a patient asked me to review her chart. Uncertain of what the “right” answer was, I asked my supervising resident who made it quite clear that patients were not allowed to just read through their medical chart in the hospital. I distinctly remember telling the patient that this was not permitted, but I also remember feeling unsettled and thinking that the paradigm was very odd – why shouldn't a patient be able to review her own medical chart? Times have clearly changed and the movement toward increased transparency in medical care continues.
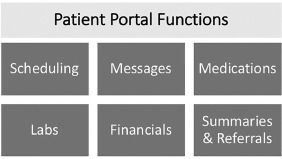
Figure 1. Common functions available on patient portals.
However, it is worth remembering that the benefit of directly providing patients with their diagnostic imaging reports may come with some unintended costs. With access to their own reports, patients will be confronted with terminology and diagnostic information for which they may have little or no training and context to interpret. Naturally, they will have their primary provider to turn to for help, though this resource may not be immediately available. Likely, they will turn to the internet, or “Dr Google,” for help. Here, patients will receive unfettered information, whether it be outdated evidence, anecdotal personal accounts, pseudo-science, and the like. Even when accessing evidence-based information, patients may not have the background to be good consumers of science – they may not be able to adequately evaluate a given research study's validity. Indeed, hundreds of research studies are published each year warning that patient education materials are written at a grade-level too advanced for most readers. If information that is intended for patient consumption is too advanced, imagine the difficulty for patients consuming information intended for physicians! Thus, a delicate balance is required to provide patients with their own health information (which is rightfully theirs to view) without placing an unintended burden on patients with this information, which if misunderstood, could lead to poor health decision making.
The target audience for our radiology reports is most certainly changing. Our reports are no longer intended solely for the referring provider. We need to be cognizant that patients may be reading our radiology reports via portal access and this raises a number of important issues that one needs to consider. The first is to diffuse any language that could be considered hostile. For example, instead of “the patient refused” the endovaginal ultrasound, one might say the “patient declined.” This is much less antagonistic to someone reading your report who has likely not had the opportunity to meet you and has only seen the line item on their healthcare bill for imaging services. Perhaps there were very good reasons to have declined the exam – we often do not know those details and it is best to use neutral language whenever possible. It is also critical to be accurate with the history you incorporate into your report – both from the electronic medical record and the history provided by the patients on their exam intake forms. We must strive to create a report, and especially an impression, that is as simple and clear as possible in order to minimize the curse of knowledge. This is helpful for both the patient and the referring provider when we create an impression in lay language rather than “radiology speak.” Perhaps instead of having the abdominal ultrasound impression read “hepatic steatosis,” we should have it read “fatty liver” which is likely to be less confusing for patients. Lastly, improvements in information technology may eventually allow us to include images and hyperlinks in reports (11), which could further improve report clarity.
CONCLUSION
In conclusion, the target audience for our radiology reports now includes our patients. This makes it even more important to strive for optimal report clarity by using structured reports, avoiding abbreviations, and addressing the clinical questions posed to us. Creating a report impression that is as simple and clear as possible and written in “lay language” is crucial to mitigating the “curse of knowledge” and “pluralistic ignorance.” Finally, teaching these reporting guidelines to our residents and fellows may prove critical to their professional success, as the ability to effectively communicate imaging findings to both providers and patients is paramount.
Funding
None
Source: Academic Radiology
Image credit: iStock, Academic Radiology
References:
1
C.E. Kahn Jr, C.P. Langlotz, E.S. Burnsides
Toward best practices in radiology reporting
Radiology, 252 (2009), pp. 852-856
CrossRefView Record in ScopusGoogle Scholar
2
L.H. Schwartz, D.M. Panicek, A.R. Berk, et al.
Improving communication of diagnostic radiology findings through structured reporting
Radiology, 260 (2011), pp. 174-181
CrossRefView Record in ScopusGoogle Scholar
3
J.M.L. Bosmans, J.J. Weyler, A.M. De Schepper, et al.
The radiology report as seen by radiologists and referring clinicians: results of the COVER and ROVER surveys
Radiology, 259 (2011), pp. 184-195
CrossRefView Record in ScopusGoogle Scholar
4
S.L. Ross, S.M. Ascher, A.S. Somwaru, et al.
Quantifying language before and after instituting structured CT reports
J Am Coll Radiol, 14 (2017), pp. 1444-1450
ArticleDownload PDFView Record in ScopusGoogle Scholar
5
B.W. Buckley, L. Daly, G.N. Allen, et al.
Recall of structured radiology reports is significantly superior to that of unstructured reports
Br J Radiol (2018), Article 20170670, 10.1259/bjr.20170670
CrossRefGoogle Scholar
6
Prentice, DA. Pluralistic ignorance. In: Encyclopedia of Social Psychology. doi:10.4135/9781412956253.n402.
Google Scholar
7
J.K. Hoang
Add value in radiology reports by providing a frame of reference
J Am Coll Radiol, 14 (2017), pp. 585-586
ArticleDownload PDFView Record in ScopusGoogle Scholar
8
C. Camerer, G. Loewenstein, M. Weber
The curse of knowledge in economic settings: an experimental analysis
J Polit Econ, 97 (1989), pp. 1232-1254
CrossRefView Record in ScopusGoogle Scholar
9
B. Lee, M.T. Whitehead
Radiology reports: what you think you're saying and what they think you're saying
Curr Probl Diagn Radiol, 46 (2017), pp. 186-195
ArticleDownload PDFView Record in ScopusGoogle Scholar
10
T. Delbanco
Open notes: doctors and patients signing on
Ann Intern Med, 153 (2010), p. 121
CrossRefView Record in ScopusGoogle Scholar
11
C.I. Lee, C.P. Langlotz, J.G. Elmore
Implications of direct patient online access to radiology reports through patient web portals
J Am Coll Radiol, 13 (2016), pp. 1608-1614
ArticleDownload PDFView Record in ScopusGoogle Scholar
12
D Henshaw, G. Okawa, K. Ching
Access to radiology reports via an online patient portal: experiences of referring physicians and patients
J Am Coll Radiol, 12 (2015), pp. 582-586
e1
View Record in ScopusGoogle Scholar
Latest Articles
Imaging, MRI, Ultrasound, Radiology, Radiologists, patient care, breast ultrasound, Radiology reports, breast screening, CT scans, patient portals, Breast Surgeon, plastic surgeons, pathologists, Structured reports, Curse of knowledge, hyperintense, precontrast, endometrioma, postcontrast, radiation oncologists, thyroid ultrasound
As the movement for increased transparency in healthcare continues, more and more patients are accessing their imaging reports via patient portals. The shift to structured radiology reports has increased report clarity for referring providers and is suppo