




Executive summary
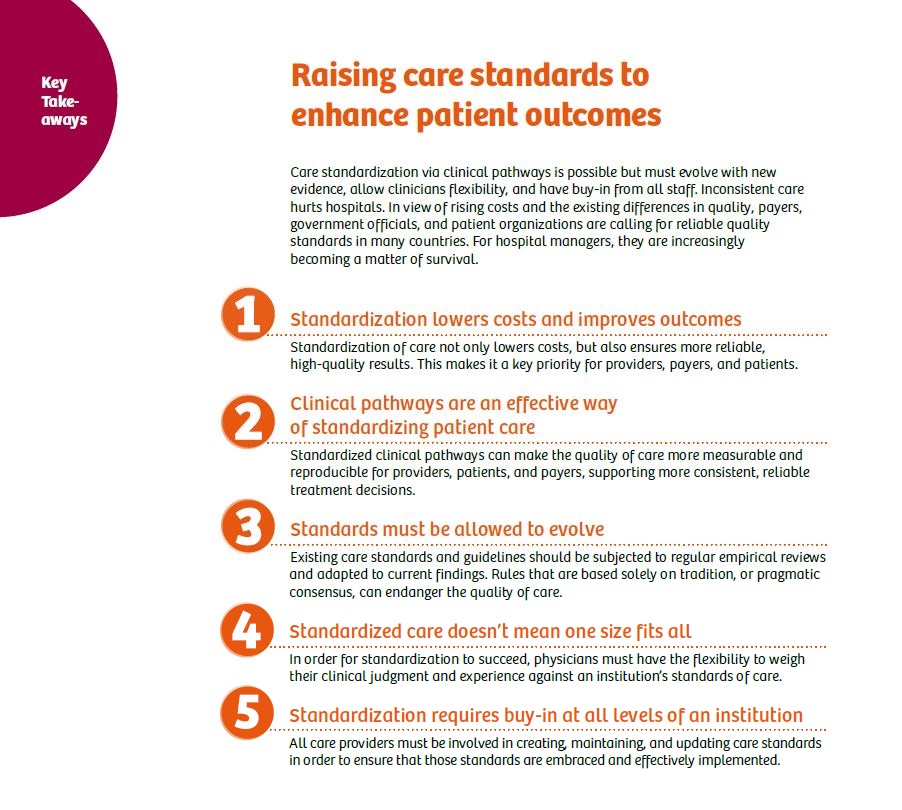
Hospitals are under increasing pressure to improve their overall quality of care. In order to contend with this challenge, many hospitals have implemented measures to establish high-quality care standards. For the most part, hospitals have elected to establish clinical pathways designed to govern the entire care process, with impressive results.
However, care standards must evolve continuously in order to remain relevant. At the same time, they must also provide healthcare practitioners with the flexibility to provide individual patients with personalized care. Furthermore, care standards require input and buy-in from the very practitioners who are charged with implementing them in order to be successful.
Introduction
Hospital reimbursements are increasingly being tied to the quality of care delivered. Care quality also affects a hospital’s reputation by either attracting or repelling patients, depending on whether the experience was perceived positively or negatively, respectively. Therefore, hospitals around the world are attempting to improve their quality of care guidelines by establishing care standards based upon the best evidence.
This white paper investigates the justification for care standardization, the methods currently being implemented to achieve it, and the elements that have resulted in the greatest amount of success. In the current environment, hospitals must consistently deliver high-quality care in order to survive.
Inconsistent quality
of care can damage hospitals’ reputations, impede the attraction of new
patients, and diminish insurance reimbursement
Patient surveys indicate that quality of care is a decisive criterion in the choice of a hospital.¹ For many years now, quality-related selection factors – such as expertise in treating a specific illness and history of medical errors – top the list from the patient’s perspective.² As such, the quality of healthcare influences occupancy and, therefore, the commercial success of a hospital.
Moreover, insurance reimbursements are increasingly being linked to objective, verifiable quality criteria, such as successfully completed surgeries, treatment efficacy, and readmission rates. Thus, poor outcomes not only detract from a hospital’s reputation, but also affect its bottom line. This has resulted in hospitals and other healthcare providers worldwide gradually attempting to apply evidence-based practices (EBPs) to these quality criteria in order to ensure that patients are being managed in an effective manner.
Even highly developed healthcare systems have challenges with delivering high quality of care consistently. In Germany, for instance, health insurance companies and patient organizations complain of the staggering quality differences between individual hospitals. Figures from the German Cancer Society (Deutsche Krebsgesellschaft, DKG) indicate that approximately 950 certified cancer centers have significantly higher survival rates than non-certified hospitals.3,4
As for the United States, if every state had the same quality of care as the highest performing state, there would have been an estimated 75,000 fewer deaths in 2005, according to a report by the Institute of Medicine at the National Academy of the Sciences.⁵ These examples highlight opportunities for improvement and illustrate why countries have moved toward standardizing care within their respective healthcare systems and organizations.
1. What is care standardization and why does it matter?
Standards are vital in many industries, from power and manufacturing to banking and mobile communications. They provide formal guidelines for procedures to support effective management and improve operational efficiency, particularly in complex industries with intricate processes.
Proven, standardized procedures can also be applied in the realm of healthcare to ensure that care is more consistent and safe for providers, patients, and payers. Poor treatment outcomes, longer hospital stays, increased readmission, damaged reputation, and even lawsuits can be avoided as a result.
“It is time for hospital leaders to move from a conventional ‘quality improvement’ focus to one of clinical standardization as a necessary first (but not last) step in improving patient outcomes,” says the U.S. Health Care Advisory Board and Physician Executive Council. “The priority now for hospital boards and executives should be to identify and reduce unwarranted variability within their own organizations.”⁶
Establishing care standards has great potential within all areas of healthcare; but focusing on a few key areas can have a particularly large impact on diminishing preventable adverse events, notes the Advisory Board. “Within the realm of acute care services, research has identified a short list of high-volume, high-variation conditions – particularly sepsis, heart failure, joint replacement, and labor and delivery (L&D) – that merit particular focus.”⁶ While the management of all hospital conditions may benefit from the establishment of care standards, focusing on standardizing these areas within acute care services can create a substantial impact.
2. Clinical pathways: A promising approach for managing quality
How does one start to standardize care? The most widespread approach for implementing standardization is through clinical pathways (also known as care pathways, critical pathways, integrated care pathways, or care maps), consisting of structured, multidisciplinary plans of care designed to support the establishment of clinical guidelines and protocols. Clinical pathways provide detailed guidance during each stage of managing a patient with a specific condition over a given period of time and include details on expected progress and outcomes. They are designed to improve the continuity and coordination of care across different disciplines and sectors.⁷
Evidence of the efficacy of clinical pathways can be found in various countries. For example, a 2014 study of cancer patients at Xi’an General Hospital in China demonstrates impressive results. In this study, a specific clinical pathway was designed to standardize the treatment of hepatectomy for patients with hepatocellular carcinoma. In all measures of postoperative outcomes – total complications, mortality, and readmissions – the results were clearly in favor of those patients who were treated according to the clinical pathway, as opposed to those patients who were not.⁸
In the United Kingdom, the National Health Service (NHS) has been working toward more transparency and EBP in medical care for many years. Tools such as the standardized Patient-Reported Outcome Measures patient survey contribute to improving the monitoring and measurement of quality of care.⁹ Likewise, the Enhanced Recovery Program (ERP), initiated by the Department of Health in 2009, illustrates the success of standard care pathways for patients in recovery.

The ERP represents an integrated care pathway composed of standardized elements before, during, and after surgery, such as preoperative therapy classes, standardized surgical and anesthetic protocols, and postoperative pain treatment. It aims to support faster, complication-free recovery and discharge of patients following elective surgery, including hip and knee replacement, major colorectal surgery, and cancer surgery.
In a study of the program’s success, the NHS Sustainable Improvement Team (formerly NHS Improving Quality) writes, “Enhanced recovery has shown its ability to improve patient experience, patient safety, and outcomes by ensuring that patients get the same standards of clinical care seven days a week. Its ability to reduce length of stay without an increase in readmissions provides real efficiency benefits for the NHS. Despite rises in activity for almost all procedures, there were nearly 170,000 fewer bed days for these procedures in 2012/13 than in 2008/09. It has been estimated that further implementation of ERPs could save up to 20,000 additional bed days per year. The ERP is now the standard care pathway for many patients having major surgery.”10
3. Standards must evolve to reflect the latest evidence 170,000 bed days saved by hospitals
Wherever standards and guidelines serve as a basis for treatment, it is important to develop them based on the best possible evidence, while also regularly reviewing them with reliable measurement tools and comparative data. However, the collection and evaluation of appropriate datasets often requires a considerable amount of additional work for employees who are already functioning under a very heavy workload. Currently, it is estimated that nurses in the United States spend only 30 percent of their time directly on patient care.⁵
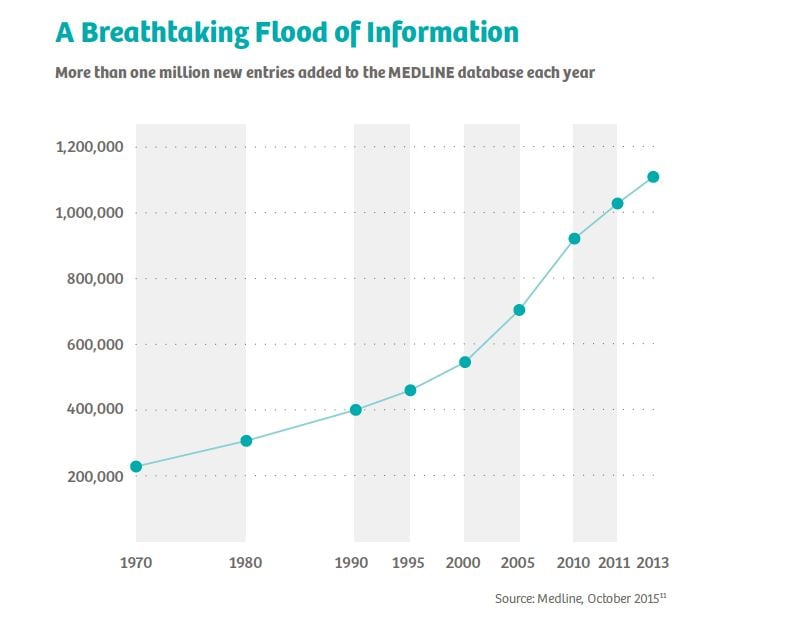
Staying on top of the rapidly evolving and expanding body of clinical evidence represents an ever-increasing challenge. For example, MEDLINE, the U.S. National Library of Medicine’s premier bibliographic database, currently contains more than 22 million references to journal articles. In the 1980s, around 250,000 to 300,000 entries were added each year. This figure has now risen to more than one million per year.11
Standardization is intended to streamline operational tasks, not provide additional administrative burdens. Helios, a German hospital chain with 111 acute-care and rehabilitation clinics and approximately 68,000 employees, has pioneered a way to integrate clinical evidence into its care standards while minimizing the burden on its staff. Helios has relied on structured quality management and continuous improvement processes for many years. As part of the Initiative for Quality Medicine (IQM), quality indicators developed by Helios for its companies at the beginning of the millennium are now being used by hospitals in Germany, Austria, Switzerland, and other countries.12 Ideally, participating providers can use the figures to compare efficiency across institutions and the IQM process to manage quality and derive optimal treatment paths.
In the interest of building the broadest and most up-to-date database possible, IQM relies on information that is already being complied, such as routinely collected billing data, thus requiring no additional data collection or administrative tasks for the hospital staff. This significantly reduces the burden on the staff and helps increase willingness to cooperate. In addition, the data is checked by third parties (e.g., health insurance companies), ensuring its quality and making it less prone to error or manipulation.
Evidence-based standards and guidelines can help doctors make decisions, avoid medical errors and omissions, explain therapeutic decisions to patients, and guarantee that all patients receive a consistently high quality of treatment. In order to promote new findings and innovative treatments, existing rules must be subject to regular empirical reviews and constantly adapted to the latest findings.
4. Balancing standardization with individualized care
Many doctors fear that standardization will restrict them in their individual treatment decisions. Likewise, patients worry that they will only get the cheapest, standardized treatment option, instead of potentially receiving more expensive, but more individualized (and possibly more effective) care.
These concerns are understandable and should be actively addressed by providers. Standardization is a multilayered issue, aimed at achieving a reliable, consistent level of quality and reducing costs. And that is in everyone’s interests.
“The goal of clinical standardization is not to produce rigid guidelines. It is to establish an evidence- and consensus-based approach that will change and evolve,” says the Advisory Board. “Nor is the goal to enforce perfect adherence. Providers should be supported in customizing for individual patient needs and innovating in ways that will end up raising the care standard over time.”6
Guidelines based on the best available evidence do not mean that a practitioner has an edict to practice in a single way. In fact, evidence alone is never sufficient to make a clinical decision about a specific patient. In order to apply evidence to a particular patient care situation, the clinician needs evidence supported by good judgment, clinical skill, and knowledge of the patient’s unique needs.
This is made particularly clear by the increasing number of patients with multiple chronic diseases. The aging of populations worldwide means that the number of elderly patients with multiple chronic conditions is increasing. In the United States alone, this affects more than 75 million people. Managing these multiple conditions requires a holistic approach, since applying the various clinical guidelines developed for single diseases may produce adverse effects.5
For example, existing clinical practice guidelines for a 79-year-old patient with osteoporosis, type 2 diabetes, hypertension, and chronic obstructive pulmonary disease can sometimes be contradictory. Osteoporosis patients are urged to do weight-bearing exercises, while diabetic patients are told to avoid them. Also, the various drugs recommended in each case may have dangerous interactions. Therefore, individual clinical decision making and different opinions about the patient’s condition will always be needed. Decisions must also continue to be made individually, and sometimes subjectively, if there is insufficient empirical knowledge to determine a specific clinical pathway.
However, guidelines should be based on more than just expert conjecture or consensus. When there is a lack of transparency in the decision-making process or inefficient sharing of data, the lack of standardization can result in challenges. In fact, varying levels of staff experience can introduce variation in the care delivery process.
Standardized operating concepts for diagnostic technology may help healthcare providers address these challenges. Automation and pre-configuration of technology, and integrated usability across assets, may help foster progress toward a value-based care environment.
5. Standardization is a team effort
In order to create and enforce standards within healthcare facilities, resolute and well-thought-out change management is required. One important prerequisite for success in standardization projects is that providers persuade everyone involved of the benefits and motivate them to participate.
Joe Landsman, President and CEO of the University of Tennessee Medical Center in the United States, reports that his institution’s staff has participated actively in the development and implementation of its care standards. “[Our] pathways are developed by multispecialty teams of our medical staff. We start with evidence-based medicine and a work redesign before we actually build the pathway, which ultimately ends up in our electronic physician order-entry system. We also have pharmacists, physical therapists, and nurses involved in the development of the pathways.” He adds, “There is rarely a decision made on this campus that the physicians haven’t had the opportunity to weigh in on. They have taken up the challenge and are developing the pathways themselves.”13
Planning for standardization should include a multidisciplinary team that has key personnel involved in patient care decisions. Gerald Hickson, M.D., Senior Vice President for Quality, Patient Safety, and Risk Prevention at Vanderbilt University Medical Center in Nashville (United States), says, “It requires a level of investment in services to support the delivery of care in the value-based world. The question is whether you, as a system, have a plan to effectively ensure adherence by all team members.”14
Reference
1. Mansky T. (2012). Was erwarten die potenziellen Patienten vom Krankenhaus? Gesundheitsmonitor 2012. Bertelsmann Stiftung und Barmer/GEK. January 1, 2012.
2. Gallup. (2005.) Healthcare panel: How do people choose hospitals? October 25, 2005.
3. AOK Bundesverband. (2015.) Krankenhaus-Report 2015: Strukturwandel der Kliniklandschaft an der Qualität ausrichten. February 20, 2015. http://aok-bv.de/imperia/md/aokbv/presse/pressemitteilungen/archiv/2015/pressemappe_komplett.pdf. Accessed February 1, 2017.
4. Deutsche Krebsgesellschaft. Das Zentrenmodell. https://www.krebsgesellschaft.de/deutsche-krebsgesellschaft-wtrl/deutsche-krebsgesellschaft/zertifizierung/das-zentrenmodel-der-dkg.html. Accessed February 1, 2017.
5. Institute of Medicine. (2012.) Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. September 6, 2012. http://www.nationalacademies.org/hmd/Reports/2012/Best-Care-at-Lower-Cost-The-Path-to-Continuously-Learning-Health-Care-in-America.aspx. Accessed February 1, 2017.
6. The Advisory Board Company. (2015.) Setting the Standard for Patient Care: Adopting a Clinical Standardization Mindset. https://www.advisory.com/research/physician-executive-council/studies/2015/setting-the-standard-for-patient-care. Accessed February 1, 2017.
7. Open Clinical. Clinical Pathways. http://www.openclinical.org/clinicalpathways.html. Accessed February 1, 2017.
8. Song, Xu-Ping et al. Could clinical pathways improve the quality of care in patients with gastrointestinal cancer? A meta-analysis. Asian Pacific Journal of Cancer Prevention 15.19 (2014): 8361-8366.
9. NHS Digital. Patient Reported Outcome Measures (PROMs). http://content.digital.nhs.uk/proms. Accessed February 1, 2017.
10. No attribution provided for this.
11. Medline (PubMed) Trend. http://dan.corlan.net/medline-trend.html. Accessed February 1, 2017.
12. Initiative Qualitätsmedizin. www.initiative-qualitaetsmedizin.de. Accessed February 1, 2017.
13. Modern Healthcare. (2015.) Standardizing care reduces costs, improves quality.
April 11, 2015. http://www.modernhealthcare.com/article/20150411/MAGAZINE/304119950. Accessed February 2, 2017.
14. HealthLeaders Media Council. (2015.) Succeeding in the Risk Era: How to Accelerate Progress Toward a Value-Based Future. January 2015. http://www.healthleadersmedia.com/report/intel/succeeding-risk-era-how-accelerate-progresstoward-value-based-future. Accessed February 2, 2017.




