
![Tuberculosis Diagnostics: The Promise of [18F]FDT PET Imaging](https://res.cloudinary.com/healthmanagement-org/image/upload/c_thumb,f_auto,fl_lossy,h_184,q_90,w_500/v1721132076/cw/00127782_cw_image_wi_88cc5f34b1423cec414436d2748b40ce.webp "Tuberculosis Diagnostics: The Promise of [18F]FDT PET Imaging")



Introduction
Hospitals around the world are under increasing pressure to improve outcomes – whether because they are operating in a fee-for-performance or value-based care environment, or simply because today’s increasingly informed patients are deliberately pursuing treatment at facilities with a reputation for superior care.
Whatever your hospital’s remuneration model may be, good treatment outcomes are essential to your success. And besides, delivering the best possible outcomes is ultimately the whole point of being a healthcare provider. So let’s take a look at possible ways to get there.
The Challenge:
Improving care can be expensive. Failure to improve it may be even more expensive.
Due to increasing cost pressures in the healthcare sector, established remuneration models for healthcare services are in transition around the world. Fees for performance and value-based systems are increasingly replacing fees for service. Major players – including Medicare and Medicaid in the United States, the National Health Service in the U.K., the National Health Care Institute in the Netherlands, and several leading European university hospitals – have all taken significant strides in this direction.1 In Germany, the proposed Hospital Restructuring Act aims for a stronger correlation between remuneration and quality of treatment. Furthermore, in newly industrialized countries, where patients pay a large share of the treatment costs out of their own pockets, the quality of treatment plays a decisive role in choosing a hospital (in addition to price and access to care).
In short, whether they are operating in a climate of value-based care or not, hospital managers around the world face the challenge of improving patients’ overall outcomes – and doing so cost-effectively. This white paper explores seven strategies that are essential for achieving better, more effective patient care.

Possible Solutions:
1. Promote more well-informed diagnoses
Every successful treatment, and path to a positive patient outcome, begins with a correct and timely diagnosis. Usually, when a patient goes to see a doctor, the first few minutes determine the subsequent treatment steps – directly influencing the success of the treatment and its cost. This makes it all the more important to have a quick and reliable decision-making process for diagnosis. Otherwise, there is risk of an unsuccessful or incorrect treatment, services being performed that are not billable, and avoidable readmissions.
However, diagnosis itself can be a particularly complex challenge. There is potential for human error, as well as errors arising from the system itself. Doctors can make cognitive errors, for example, by fixating on a specific diagnosis too quickly and ignoring or misinterpreting contradictory data and information for too long. The larger healthcare system may also contribute to diagnostic errors through the loss of information, delays, or misunderstandings when forwarding information – both within a hospital and to external facilities providing subsequent treatment.
Dramatic system-related errors can arise from diagnostic imaging, when images acquired don’t resolve the referring clinician’s diagnostic questions. Moreover, several studies have demonstrated that images can frequently be misinterpreted. For instance, a U.S. study observed mammographies over a 10-year period and found that more than half of cancer-free women were called back for more tests because of a false-positive result, while about one in 12 women received a false-positive biopsy recommendation.3 Outdated equipment with inadequate image quality can also lead to misdiagnosis.
Diagnostic errors are relatively common in other areas as well. Research suggests that diagnostic errors affect one in 20 patients in the United States annually, impacting an estimated 12 million Americans every year.2 Moreover, diagnostic error is the leading cause of medical malpractice claims in the United States (almost 30 percent) and is estimated to cause 40,000-80,000 deaths annually.2
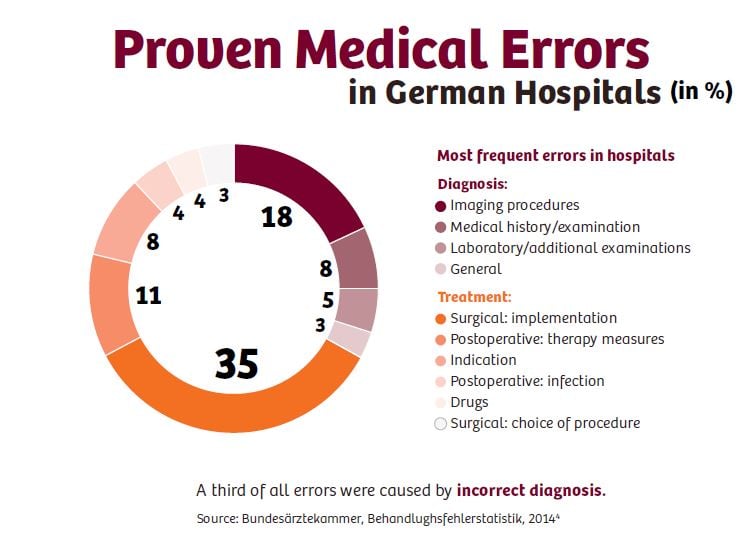
In Germany too, diagnostic error is among the most common causes of patient complaints. In 2014, the German Medical Association received around 13,700 patient complaints, of which more than one-fifth were for alleged misdiagnoses. In total, the evaluators attested to a treatment error in around 2,200 cases in 2014. One-third of them were caused by an incorrect diagnosis.⁴
As demanding as it is to try to identify and prevent the causes of diagnostic errors, it is well worth the effort, as it can significantly improve patient outcomes. Misdiagnosis can result in unnecessary treatment of non-existing conditions or proper treatments being provided too late (or not all). This impacts not only patients but providers as well. Providers are increasingly facing the operational and economic consequences of incorrect medical care. For instance, when lengths of stay are unnecessarily long, medications are sometimes used incorrectly, or avoidable exams and operations are performed. This often worsens the patient’s condition, increases readmissions, reduces efficiency, and, in the worst cases, causes expensive legal battles.
In some cases, diagnostic errors may be caused by staff shortages, time pressure, or temporary overwork. The goal is, of course, to prevent these from happening. A modern software-based workforce management system can help optimize the organization of in-house resources. Furthermore, robust hospital information systems and innovative user-friendly diagnostic tools can help reduce errors and lead to faster diagnoses. Going forward, we can expect to see knowledge-based IT systems substantially supporting decision-making and quality assurance in diagnosis.
2. Support optimal treatment planning
Usually, diagnostic procedures are followed by a treatment decision, and for most diagnoses, there are multiple possible treatment options. Selecting the right approach for a given patient can have a significant impact on the outcome. The increasing use of clinical pathways, fueled by evidence-based practices, can help encourage practitioners to implement treatment strategies that have been proven to yield better results at a lower cost.
However, sound treatment planning remains especially challenging with patients who suffer from several diseases at the same time or who suffer from a rare or complex disorder (for which advances in diagnosis have often outpaced advances in treatment). Across the European Union, approximately 30 million people suffer from one of the 8,000 rare medical conditions currently known and recognized, for which treatment options are often still insufficiently researched.⁵ Here, too, advanced technology can make a difference.
For instance, the increasing use of Electronic Health Records (EHRs), along with a seamless flow of information between physicians and specialists – and between science and technology – can play a crucial role in ensuring that clinicians are aware of patients’ comorbidities and that they exercise caution when implementing treatments that would be obvious choices for more conventional patients.
Additionally, powerful monitoring, diagnostic imaging, and laboratory equipment increasingly support the ongoing, real-time assessment of treatment success – including providing intraoperative guidance. Clinical monitoring will become more and more important in optimizing patient outcomes and maximizing cost efficiencies.
However, many hospitals avoid investing in modernization or delay purchasing expensive equipment. For many providers, increasing cost pressure can delay or even prevent adequate investment in technology. This creates significant national differences in hospital equipment between richer and poorer countries.
This is shown, for instance, in the data on equipment stocks regularly surveyed by the COCIR, the European Trade Association representing the medical imaging, health information and communications technology, and electromedical industries. The figures show that patients across Europe, especially in Eastern Europe, have very unequal access to MR or CT scanners. Moreover, in many European countries, the installed equipment base is the oldest that it has ever been. For example, more than 60 percent of the CT scanners installed in Greece or Spain are more than five years old and around one-fifth of them have been in operation for ten years or longer.⁶
While economic realities can’t be ignored, it must also be recognized that delays in investing in up-to-date technology can have a measurable opportunity cost in terms of worse patient outcomes, and consequently, decreased reimbursements and revenues.
3. Take good care of your clinicians
It has become increasingly evident that the atmosphere and working conditions within a hospital can have a profound impact on patient outcomes.
For instance, a study of nurse practitioners’ environments in the United States observed a strong correlation between better care environments (i.e., better staffing, investments in staff development, quality management, frontline manager supervisory ability, and good relations with physicians) and reduced patient mortality.7
This point is reinforced in a 2008 review of the international evidence concerning the correlation between nursing practice environments and patient outcomes. One of the evaluated studies noted significantly better outcomes among hospitals that were awarded Magnet status, an award given by the American Nurses Credentialing Center to hospitals that satisfy a set of criteria designed to measure the strength and quality of their nursing department. The authors attributed this difference in outcomes to organizational features through which nurses experienced greater autonomy, more control over their practice, and better relationships with physicians.8
This same review also considered a survey of 43,000 nurses in 700 hospitals in the United States, Canada, England, Scotland, and Germany. The surveyed nurses agreed that while their working relationships with physicians were largely positive, their hospitals generally didn’t provide the support services that the nurses needed to get their jobs done, and fewer than half of the respondents felt that their hospital administrators listened and responded to their concerns. Authors Robyn B. Cheung, et al., concluded that their study’s findings “provide convincing evidence of the crucial role that staffing ratios, and administrative and managerial support, play in the quality of patient care and patient outcomes.”8
On a related note, a 2009 survey by the American College of Physician Executives found that many hospitals have a culture of tolerating “disruptive behavior,” such as unprofessional outbursts and overreactions, and that such a climate can have a detrimental effect on outcomes. The results included a somewhat extreme example of a nurse who witnessed the onset of complications in an intensive care patient, but refused to contact the on-call physician due to being afraid of his temper. At least one observer believed that this delay contributed to the patient’s death. Fairly egregious behaviors – such as making degrading comments and insults, yelling, cursing, inappropriate jokes, and refusing to work with or speak to colleagues – were found to be fairly common. Less common (but still troubling) behaviors included throwing objects, spreading malicious rumors, and trying to get colleagues unjustly disciplined, or even fired.9
It seems obvious that such disruptive behaviors would have a negative impact on patient care. A 2006 survey published in the Journal of the American College of Surgeons substantiates this conclusion. Sixty-eight percent of operating room staff believed that disruptive behaviors impaired the quality of care; 67 percent said that these behaviors contributed to adverse events or medical errors; 58 percent thought such behaviors compromised safety; and 28 percent felt that disruptive behaviors had contributed to patient mortality.10
“Culture manifests itself in the collective behaviors of the workforce,” wrote hospital administrators Bryan J. Warren and Rhonda Larimore, “so the desired behaviors need to be identified and encouraged, and detrimental behaviors cannot be tolerated.” They added, “This sounds simple enough in theory, but adhering to this principle in the face of tradition and short-term pressures is a challenge.”11
While changing the culture of an organization may be difficult, a case study published by consulting firm B.E. Smith demonstrates that it can be done. Two emergency departments (EDs) within a dual-campus, non-profit, community-based healthcare system suffered from a culture in which relationships between the emergency care team and inpatient care providers were poor, leading to communications that seemed adversarial rather than collaborative. This created tension between the EDs and inpatient departments and negatively impacted the organization’s overall performance.
The consultants worked with the staff to develop a culture in which patients were viewed more as customers and attempted to instill a better understanding of how the EDs fed the inpatient setting and vice versa – and how this supported the successful financial health of the organization as a whole. This contributed to the implementation of a strategy to create an “ED without borders.” The consultants built a process improvement team with representation from the emergency department, nurses, medical staff, ancillaries, and C-suite executives. This cross-disciplinary teamwork helped the staff develop a shared sense of focus and urgency when it came to understanding the ED’s role in the overall patient care process. This process improvement exercise ultimately led to significant reductions in turnaround time and the capture of previously lost revenues.12
In short, the working climate within a hospital matters and has an impact on patient outcomes. Every hospital administrator wishing to improve outcomes should take a keen interest in the hospital’s working atmosphere and strive to address negative dynamics, while reinforcing positive ones as proactively as possible.
4. Improve outcomes through greater transparency
As described in the previous sections, the quality of diagnoses, treatment decisions, and treatment monitoring can significantly affect patient outcomes. But healthcare providers must also ensure that their outcome results are transparent in order to hold their own in the increasingly competitive environment over patients, contracts with payers, and/or public resources. “Provider organizations understand that, without a change in their model of doing business, they can only hope to be the last iceberg to melt. Facing lower payment rates and potential loss of market share, they have no choice but to improve value and be able to prove it,” writes economist Michael Porter in the Harvard Business Review.13
However, this is easier said than done. Although hospital managers have now recognized the need for transparent and complete outcomes reporting, in practice they often lack suitable measurement methods. Most quality metrics do not gauge quality; rather, they are process measures that capture compliance with practice guidelines. Take, for example, the Healthcare Effectiveness Data and Information Set (HEDIS) that is used by the vast majority of American health plans to measure performance of care. HEDIS scores consist entirely of process measures, as well as easy-to-measure clinical indicators that fall far short of actual outcomes. For example, HEDIS covers data on immunizations, checkups, medication, or diagnostic procedures – rather than the actual results of treatment.14
The Boston Consulting Group (BCG) consultants, Elisabeth Hansson, Arne Kohler, Nicolai Skarsgård, and Stefan Larsson, have made a similar observation. “We can measure many things as we try to understand the quality and efficiency of healthcare, but very few conventional metrics currently tracked by providers reflect actual health outcomes,” the authors write.1
The BCG authors in no way deny the importance of many hospital metrics gathered worldwide: All of these conventional metrics play an important role in healthcare. They provide vital data and, when strongly correlated with outcomes, ensure a powerful and balanced set of metrics, says the article. However, it also points out that when used in isolation, without an adequate focus on outcomes, such metrics can be misleading and can prevent management and clinical teams from focusing on what’s most important.1
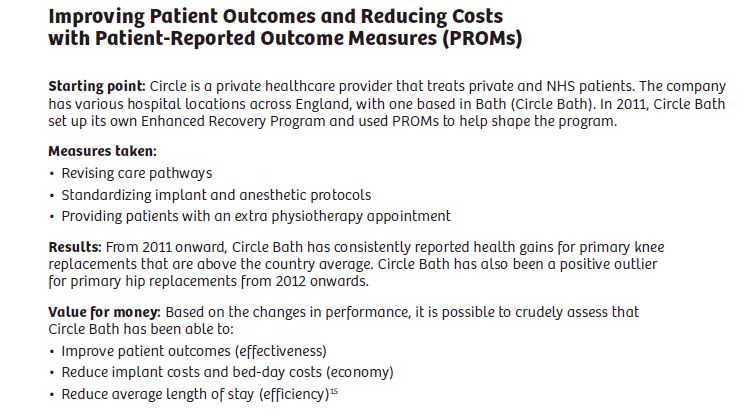
To gain meaningful benchmarks, care providers should therefore actively engage patients in the collection of outcomes data. Patient-Reported Outcome Measures (PROMs) are already successfully being used by various hospitals in the United Kingdom to improve patient outcomes. The National Health Service (NHS) launched a corresponding project in 2009. PROMs are used to calculate the health gains after several forms of surgical treatment, using preoperative and postoperative surveys. Patients undergoing surgery for four common elective procedures (hip and knee replacement, varicose vein surgery, and groin hernia surgery) are asked to complete questionnaires before and after their operations to assess their improvement in health. The results are regularly evaluated and published.
In a study, Britain’s Health and Social Care Information Centre (HSCIC) compiled a number of successful examples showing how hospitals have successfully used the PROMs data as a benchmark for their own quality measures. The Best Case Studies published by the HSCIC led to the conclusion that standardization can greatly help improve patient outcomes. At the same time, the case studies suggest that improved patient outcomes do not necessarily have to be accompanied by higher costs, but can even improve profitability.15
To measure is to learn, believes the International Consortium for Health Outcomes Measurement (ICHOM).17 The non-profit organization has defined outcomes as the results people care about most when seeking treatment, including functional improvement and the ability to live normal, productive lives. Its founding members include BCG, the Harvard Business School, and Sweden’s renowned Karolinska Institutet, a medical university in Stockholm.
The ICHOM defines and publishes international standards for measuring outcomes. It has already published 12 sets of standards for widespread global conditions, including coronary artery disease, prostate cancer, lower-back pain, depression, and Parkinson’s disease. Seven more are in development. The aim is to obtain international benchmarks data derived from standardized, internationally accepted, metrics that enable care teams across the world to learn from one another. Measuring and reporting outcome data allows caregivers in any country to evaluate their work using the universal “language of health outcomes.”16
5 Ensure continuity of care following discharge
Particularly in Western industrialized nations, the present-day healthcare organization is a highly sophisticated, but fragmented, collection of service providers. Previously, following a patient’s case often ended at the point of transfer (to another provider/specialist) or discharge. Follow-up on the success of treatment rarely took place.
In view of rising costs, however, payers in many countries are increasingly seeking to make optimum use of available healthcare resources. To ensure more cost-effective healthcare, providers are examining the entire care continuum for improvements. By embracing the overall patient journey, providers can potentially improve patient outcomes, while reducing costs.
The 2010 Affordable Care Act launched in the United States included financial incentives for providers to continue making a positive contribution to patient outcomes beyond the day of discharge. For instance, Medicare reduces provider compensation if patients are readmitted within 30 days of discharge. This affects one in every five Medicare patients – a staggering number of those treated. According to Kaiser Health News, 2,597 of the 3,400 Medicare contract hospitals faced cuts totaling more than $500 million in fiscal year 2016 due to such readmissions.17
The continuing trend toward managed care programs in the United States and other countries is also driving provider cooperation and alliances. Integrated healthcare delivery systems that encompass hospitals, physician groups, ambulatory clinics, and other provider facilities are on the rise. This is a positive development for patient outcomes. After all, other service sectors have long since adopted the principle of focusing on the customer, systematically aligning the organization to customer needs to create a consistently positive user experience.
To summarize, it is in the hospitals’ best interest to foster communication, coordination, and follow-up with the rehabilitation centers, specialists, and general practitioners into with whom their patients see, even after they are discharged.
6. Engage and support your patients after discharge
Survey and research results show that hand-off communication and the discharge process are sorely in need of improvement in many hospitals – not just with other healthcare practitioners, but also with the patients themselves. For instance, in the United States’ latest annual national patient survey, the CAHPS Hospital Survey,14
14 percent of respondents said they neither received any written information about what symptoms or health warning signs they should look for in the future, nor had conversations about the need for a follow-up appointment after their discharge.18 Clearly this is a breakdown that could have significant consequences for patient outcomes.
However, engaging with patients can be challenging. Socioeconomic factors, such as low income, unemployment, and poor education, can lead patients to neglect their health and fail to follow their doctors’ recommendations or keep appointments. Several studies from the United States actually show a link between high readmission rates and a hospital’s catchment area. The research findings suggest that hospitals in economically disadvantaged regions are disproportionately affected by readmission penalties.20 This, once again, shows how important it is to develop reliable and reasonable outcome measurements – not just for providers who are affected by severe cuts, but also to improve patient care in more problematic areas.
7. Use connected care to support better outcomes
A well-managed IT infrastructure, along with mobile technology, could help smooth the patient pathway and enforce patient engagement. The Veterans Health Administration (VHA), the biggest integrated health network in the United States, recently started using mobile resources like tablets and smartphone apps to help VHA doctors and patients stay connected. In other words, visit-based care is giving way to connected care. “I think of connected health as a wave that’s just forming, and that will crest over the next decade,” says Dr. Kevin Vigilante, Senior Vice President of Booz Allen Hamilton, the consultancy that is supporting the VHA pilot project.21
In developed economies, some of the greatest benefits of connected care could result in improved treatment of chronic disease. Furthermore, the greatest benefits of Internet of Things (IoT) applications could be in expanding delivery of healthcare services to the underserved, write the corporate consultants at McKinsey in a recent study.22 For example, it may become more possible to diagnose hypertension in rural China or help diabetics in India avoid complication with IoT-based mobile services. Permanent remote monitoring of patients via mobile apps (or perhaps even future smart pills or implants) could enable more timely interventions, help patients to consistently comply with prescribed treatments, or motivate them to change their lifestyles for the sake of better outcomes.
The EHRs that have been introduced in many countries also provide a shared platform for decision-making among patients and doctors. According to a recent survey by the consulting firm Accenture, more than half of all patients want to be able to access their data online.23 This would definitely benefit many doctors. A vast majority of United States doctors report that patient updating of personal electronic medical records improves patient engagement and satisfaction.24 Healthcare providers who manage to create stronger ties to their patients and let them independently contribute to their patient journey can achieve better long-term patient outcomes.
Key Take-aways:
In an era of value-based care, outcomes matter more than ever. Improving outcomes is achievable and vital for hospitals’ survival.
1. Promote more well-informed diagnoses
An accurate and quick diagnosis is an essential aspect of improving patient outcomes. It is the foundation for proper treatment decisions. IT plays a significant and growing role in processing diagnosis-relevant patient information in a comprehensive and purposeful way. Modern diagnostic exams help increase diagnostic quality, thereby reducing downstream costs resulting from misdiagnoses.
2. Support optimal treatment planning
Treatment can be efficient without being effective, and vice versa. Ensuring that treatment is both efficient and effective is the hallmark of medically and economically successful healthcare providers.
3. Take good care of your clinicians
An antagonistic work atmosphere for clinicians and nurses translates into inferior outcomes for patients. Providing a supportive workplace environment leads to happier employees, which in turn yields better patient care.
4. Improve outcomes
through greater transparency
To ascertain the success of improvement measures, patient outcomes must be clearly defined, reliable, and transparently evaluated. True measures of quality should reflect what matters to the patient.
5. Ensure continuity of care following discharge
The seamless flow of information along the treatment pathway is an essential component in the overall success of the treatment. Especially when it comes to hand-offs, there is often still room for improvement. It is key that hospital operators provide comprehensive, prioritized, and systematic information to subsequent treatment providers.
6. Engage and support
your patients after discharge
More positive patient outcomes can be achieved if patients are actively involved in the treatment process. Clear, intelligible communication is the key to success.
7. Use connected care to support better outcomes
Modern, connected IT, as well as the use of mobile devices, can contribute enormously to advances in diagnostics and treatment. This is especially true for regions of the world that are still medically under-served.
References
- Hansson E, Kohler A, Skarsgård N, Larsson S. (2015.) How to define health care outcomes. BCG Perspectives. September 21, 2015. https://www.bcgperspectives.com/content/articles/health-care-payers-providers-how-to-define-health-careoutcomes/. Accessed April 2, 2017.
- Society to Improve Diagnosis in Medicine. (2016.) About diagnostic error. http://www.improvediagnosis.org/page/AboutDiagnosticErr. Accessed April 2, 2017.
- Hubbard RA, et al. (2011.) Cumulative probability of false-positive recall or biopsy recommendation after 10 years of screening mammography. Annals of Internal Medicine. October 18, 2011. 155(8):481-492.
- German Medical Association. (2014.) Statistische Erhebung der Gutachterkommissionen und Schlichtungsstellen für das Statistikjahr 2014. http://www.bundesaerztekammer.de/fileadmin/user_upload/downloads/pdf-Ordner/Behandlungsfehler/Behandlungsfehlerstatistik.pdf. Accessed April 2, 2017.
- Nationales Aktionsbündnis für Menschen mit Seltenen Erkrankungen NAMSE. http://www.namse.de/seltene-erkrankungen.html. Accessed April 2, 2014.
- COCIR. (2014.) Medical imaging equipment: Age profile & density. http://cocir.org/uploads/media/14008_COC_Age_Profile_web_01.pdf. Accessed April 2, 2017.
- Aiken LH et al. (2008.) Effects of hospital care environment on patient mortality and nurse outcomes. Journal of Nursing Administration. May 2008; 38(5):223-229.
- Cheung RB et al. (2008.) Nursing care and patient outcomes: International evidence. Enfermeria Clinica. 2008; 18(1):35-40.
- Johnson C. (2009.) Bad blood: Doctor-nurse behavior problems impact patient care. Physician Executive. Nov-Dec 2009; 35(6):6-11.
- Rosenstein AH, O’Daniel M. (2006.) Impact and implications of disruptive behavior in the perioperative arena. Journal of the American College of Surgeons. July 2006. 203(1):96-105.
- Warren BJ, Larimore R. (2012.) How culture drives, or hinders, hospital outcomes. Select International. http://www.selectinternational.com/whitepaper-how-culturedrives-hospital-outcomes/. Accessed April 3, 2017.
- B.E. Smith. Case study: Leadership and collaboration improve ED turnaround. https://www.besmith.com/trends-and-insights/articles/. Accessed April 3, 2017.
- Porter ME, Lee TH. (2013.) The strategy that will fix health care. Harvard Business Review. October 2013. https://hbr.org/2013/10/the-strategy-that-will-fix-healthcare Accessed April 2, 2017.
- National Committee for Quality Assurance. (2015.) HEDIS 2015. http://www.ncqa.org/hedis-quality-measurement/hedis-measures/hedis-2015. Accessed April 2, 2017.
- Basser MR. (2015.) Benefits case study: “Patient Reported Outcome Measures (PROMs)” outputs: Improving health outcomes for patients undergoing knee replacement, hip replacement, varicose vein and groin hernia treatments. Health and Social Care Information Centre (HSCIC). August 20, 2015.
- International Consortium for Health Outcomes Measurement (ICHOM). Why measure outcomes? http://www.ICHOM.org/why-measure-outcomes. Accessed April 2, 2017.
- Rau J. (2016.) Medicare’s readmission penalties hit new high. Kaiser Health News. August 2, 2016. http://khn.org/news/more-than-half-of-hospitals-to-be-penalizedfor-excess-readmissions/. Accessed April 2, 2017.
- Summary of HCAHPS survey results: July 2013 to June 2014 discharges. http://www.hcahpsonline.org/Files/Report_April_2015_States.pdf. Accessed April 2, 2017.
- Joint Commission Center for Transforming Healthcare. Facts about the hand-off communications project. http://www.centerfortransforminghealthcare.org/assets/4/6/CTH_HOC_Fact_Sheet.pdf Accessed April 2, 2017.
- Barnett ML, Hsu J, McWilliams JM. (2015.) Patient characteristics and differences in hospital readmission rates. JAMA Internal Medicine. November 2015. 2015;175(11):1803-1812.
- Vigilante K, Crowe R. (2015.) Unleashing mobile technology to enable continuous care: Changing healthcare delivery for our nation’s veterans. Booz Allen Hamilton. https://www.boozallen.com/c/insight/thought-leadership/connected-health.html Accessed April 2, 2017.
- Manyika J et al. (2015.) The internet of Things: Mapping the value beyond the hype. McKinsey Global Institute. June 2015. http://globaltrends.thedialogue.org/publication/the-internet-of-things-mapping-the-value-beyond-the-hype/. Accessed April 2, 2017.
- Accenture. (2015.) Top 5 eHealth Trends. https://www.accenture.com/us-en/insight-ehealth-trends-report. Accessed April 2, 2017.
- Accenture. (2015.) Doctors survey 2015. https://www.accenture.com/au-en/_acnmedia/Accenture/Conversion-Assets/DotCom/Documents/Local/en-gb/PDF




