



1.1 Background
Ultrasound is a standard way to evaluate fetal anatomies. For the examination of fetal brain, one of the most important anatomical views is median sagittal plane (MSP).This plane can provide unique information of intracranial structures such as corpus callosum (CC) and cerebellar vermis (CV). Several studies[1~6] have proved that median sagittal plane plays an critical role in clinical diagnoses, especially for diagnosing agenesis of corpus callosum(ACC) and Dandy-Walker syndrome. Unfortunately, because of fetal position, acoustic shadow and the differences among sonographers’ scanning skill[4], MSP is particularly difficult to obtain in 2D ultrasound. Xie et al[5] showed that the percentage of successfully acquiring fetal sagittal plane from 2D ultrasound is only 35.5%. Due to the low acquisition rate of MSP with 2D scanning, many clinicians only use the brain transverse sections to do indirect diagnosis, leading to very high misdiagnosis rate of the CC or CV related diseases.
Nowadays, three-dimensional (3D) ultrasound has been widely applied to fetal examination; one of the advantages lies in the capability of obtaining any section from a volume data. Actually it is not an easy job to do so because one should not only tune many rotaries and buttons but also have a good spatial imagination in mind. In fact, only a few doctors can manually obtain fetal MSP from 3D ultrasound volume dataset in practice. Even so, such manual operation is indeed time-consuming. According to a recent report[6], for a skilled sonographer, manual acquiring MSP usually takes about 65s~186s, with the average time of 90.7±8.6s.
So a quick and easily handled tool to get MSP would be much helpful for clinical diagnosis.
1.2 Smart MSP Introduction
1.2.1 Workflow
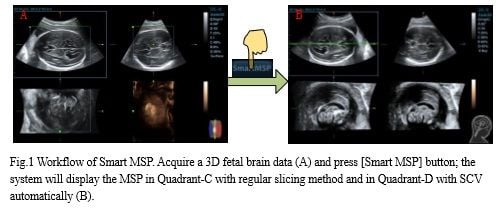
In order to obtain fetal MSP quickly and accurately, Mindray has developed an innovative software named “Smart MSP” (available in DC-8Exp and DC-8 V4.0) to detect and display MSP automatically. The workflow of Smart MSP is as follows:
- Obtain a 3D fetal data using the transverse plane as the start plane (recommend to use the transthalamic plane).
- Press [Smart MSP] button, the system will detect and display the MSP in Quadrant-C automatically.
Fig.1 is the workflow of Smart MSP. Users can measure some objects of interest in MSP, including:
i) the craniocaudal diameter, the anteroposterior diameter and the surface area of cerebellar vermis (CV),
ii) the length of corpus callosum (CC) and so on. These measurements are often related to the gestational age. Vinals F et al [1] proposed a relevant curve between CV related measurements and gestational age from the statistics of a large number of clinical data. Users can refer to this paper to evaluate whether the measured values are normal or not.
Some studies[1] shows that rendering MSP with certain thickness can improve the image contrast resolution which is helpful to observe CC and CV, so we also display MSP with SCV (slice contrast view) in Quadrant-D to improve image contrast resolution. Fig.1 (B) is the UI of Smart MSP. Specifically, Quadrant-C displays the MSP with regular slicing method and Quadrant-D displays the MSP with SCV.
1.2.2 Method
In transverse sections, we can see there is a bright line in fetal brain which is called midline in clinical. In current 3D systems, if we rotate midline to the horizontal position in Quadrant-A and put the reference point to the midline, the median sagittal plane will display in Quadrant-C. So the key of this method is to learn the feature of median sagittal plane and detect the position of median sagittal plane from a huge searching area. Fig.2 shows the spatial relationship of the fetal brain. Quadrant-A is the transverse plane as the midline is clearly shown. Quadrant-B is the plane which perpendicular to the Quadrant-A as another midline is also shown. The midlines shown in both Quadrant-A and B determines the position of MSP.
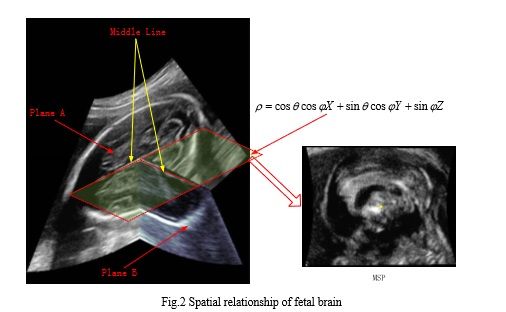
In mathematics, the plane equation can be expressed as:
ρ=cosƟ cosɸX+ sinƟ cosɸY+sinɸZ
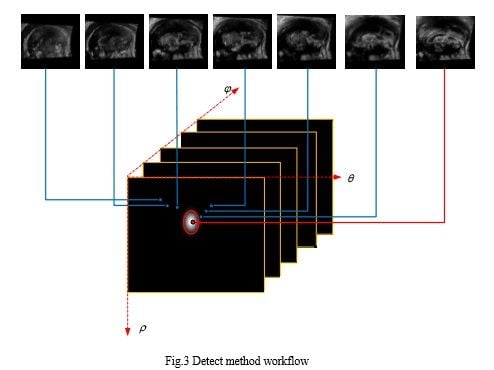
The plane equation contains 3 parameters[ρ,Ɵ,ɸ], so the aim of Smart MSP is to find out the appropriate parameters [ρ,Ɵ,ɸ] that can fit the MSP best. A novel method based on pattern recognition is proposed to calculate the plane parameters efficiently and accurately. Fig.3 shows the workflow, for each possible candidate of parameters, we calculate the likelihood of MSP and choose the max likelihood as the best fitting parameters.
1.3 Case Study
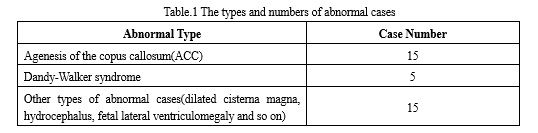
Smart MSP was clinically validated over 235 cases in Shenzhen People Hospital, China. Specifically, the cohort of clinical trial consists of 200 normal cases and 35 abnormal cases. These abnormal cases include agenesis of the copus callosum (ACC) cases, Dandy-Walker syndrome cases, dilated cisterna magna cases and so on (see Table.1). The success rate of MSP acquisition is up to 95% for normal cases and 85% for abnormal cases using Smart MSP. All the abnormal cases and a part of normal cases were also verified using MRI, and the diagnosis based on Smart MSP well accorded with the MRI findings.
The followings are some case studies:
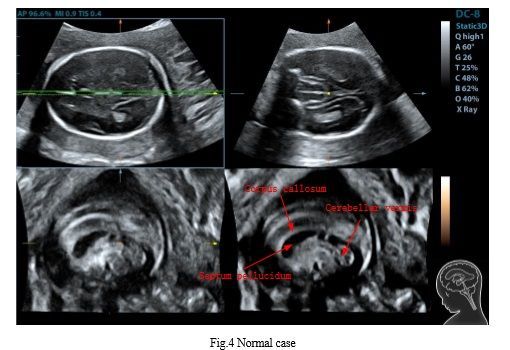
- Case 1: Normal case GA:20W5D Age:31
This is a normal case as the cavum septi pellucidi, corpus callosum, cerebellar vermis clearly and the size of these structures is normal.
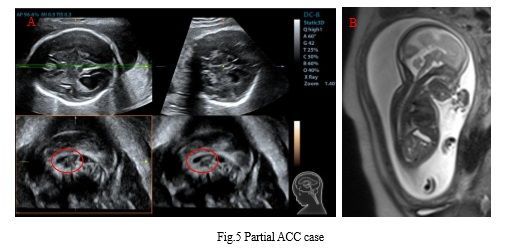
- Case 2: Partial ACC(partial Agenesis of the copus callosum) case GA:24w0D Age:32
This is a partial ACC case as the cavum septi pellucidi is very small and the length of corpus callosum is very short. Moreover, this case is accompanied with dilation of bilateral ventricle (Fig.5 A). MRI confirmed these findings (Fig.5 B).
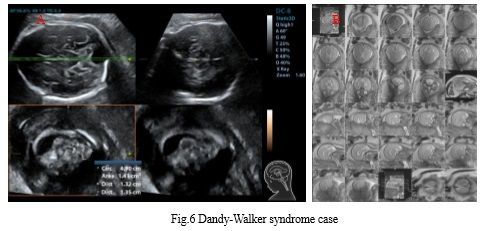
- Case3: Dandy-Walker syndrome GA:29W0D Age:31
This is a Dandy-Walker syndrome (cerebellar vermis hypoplasia) case as the size of cerebellar vermis is smaller than normal (Fig.6 A). MRI confirmed these findings (Fig.6 B).
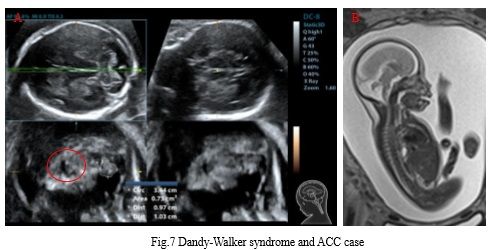
- Case 4: Dandy-Walker syndrome and ACC GA:24W0D Age:32
This fetus had both Dandy-Walker syndrome and ACC. The size of cerebellar vermis is smaller than normal. What's more, the cavum septi pellucidi is very small and the length of corpus callosum is very short (Fig.7 A). MRI confirmed these findings (Fig.7 B).
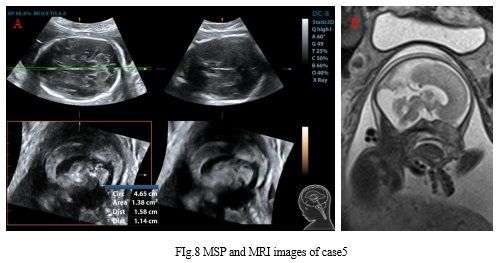
- Case 5: Misdiagnosis as Dandy-Walker syndrome in 2D but correct diagnosis from Smart MSP GA :24w0 D Age:33
This fetus was diagnosed as Dandy-Walker syndrome from 2D ultrasound in some other hospital. However, after acquiring the MSP using Smart MSP when the patient came to Shenzhen People Hospital for further diagnosis, the cerebellar vermis was found and the size was normal which means the fetus vermis was indeed normal and was misdiagnosed using 2D ultrasound (Fig.8 A). The patient was further asked to have a MRI scan which also confirmed the findings using Smart MSP (Fig.8 B).
1.4 Operation Tips
- Recommended gestational age: 20~30 weeks
Some structures may not fully developed if the gestational age is below 20 weeks while some structures may easily shaded by acoustic shadow if the gestational age is above 30 weeks. Both are not suitable for diagnosis.
- Brain middle line angle
The brain middle line angle relative to the horizontal plane should be less than 40° in the start plane of scanning. Ultrasound is easier to show the target which perpendicular to the beam, so if the angle is too large, the display of midline structures may not be ideal.
- ROI size
ROI size is recommended to be adjusted just enough to cover the skull (see Fig.9); however, the ROI size should not be too large as this will lead to a scan with too much unrelated information which will degrade the image resolution.

- Other tips
During 3D acquisition, user is recommended to observe the 3D acquisition procedure to insure no acoustic shadow in the scanning planes. Making the midline slightly tilted and the cerebellar side up can effectively avoid the acoustic shadow.
1.5 Conclusions
Mindray provides a robust solution of automated extract of fetal MSP through Smart MSP. The methodology was specifically designed to enable the detection of MSP with both precision and speed (less than 1 second). The clinical trials have demonstrated Smart MSP can significantly simplify the process of acquiring MSP and assist doctors with efficient and accurate diagnosis.
References:
[1] Vinals F, Munoz M, Naveas R, Schalper J, Giuliano S, The fetal cerebellar vermis: anatomy and biometric assessment using volume contrast imaging in the C-plane(VCI-C), Ultrasound Obstet Gynecol, 2005.
[2] D'Addario V, Pinto V, Di Cagno L, Pintucci A. The midsagittal view of the fetal brain: a useful landmark in recognizing the cause of fetal cerebral ventriculomegaly. J Perinat Med, 2005.
[3] Chang C, Chang F, Yu C, Ko H, Chen H. Three dimensional ultrasound in the assessment of fetal cerebellar transverse and antero-posterior diameters. Ultrasound Med Biol, 2000.
[4] Pilu G, Segata M, Chi T,Carletti A, Perolo A, Santini D, Bonasoni P, Tani G, Rizzo N, Diagnosis of midline anomalies of the fetal brain with the three-dimensional median view, Ultrasound Obstet Gynecol, 2006.
[5] Xie H, Cai D, Zhu Y, Li L, Study on the development of fetal cerebellar vermis with the third plane image of three-dimensional ultrasonography. Chinese Journal of Ultrasound in Medicine, 2006.
[6] Yang J, Yuan J, Qu X, Three-dimensional ultrasound visualization for fetal corpus callosum and cerebellar vermis midline image, Chin J Med Imaging Technol, 2012.
Latest Articles
Ultrasound, MIndray, Sonography, MSP
Ultrasound is a standard way to evaluate fetal anatomies. For the examination of fetal brain, one of the most important anatomical views is median sagittal plane (MSP).
















