




ICU Management & Practice, Volume 21 - Issue 2, 2021
 PRINT OPTIMISED
PRINT OPTIMISED
1. Make the patient the centre of our preoccupations
This is the first principle of wellbeing in the ICU and should be written in large letters when one enters an ICU. Wellbeing must concern first and foremost the patient. The patient should be positioned, figuratively, at the centre of the ICU room, with the focus of all members of the ICU team, including close friends and relatives, directed towards them. The purpose of this whole team is, after all, to improve the patient’s health and wellbeing, both physical and mental, remembering that good end-of-life care is an important aspect of ensuring patient wellbeing; not all patients will survive, but non-survivors must be allowed to have a dignified death (Figure 1).
2. Use the full potential of bedside rounds
Attending rounds for just 10 minutes can give a good overall impression of the quality of patient care on that ICU and of staff wellbeing. Rounds need to be instructive and effective. They should focus on relevant, new information, using terms that everybody, patient and family included, can understand. Rounds should be conducted at the right pace: not wasting time, but not rushing either; offering some teaching, but not too much as time is limited. The same historical elements of a patient’s course do not need to be repeated every day. To improve efficiency, presentations should be structured, using a problem list and considering aspects of the SOAP construct: Subjective (how the patient feels), Objective (relevant clinical and other data, including consultant’s opinion), Assessment (putting everything together), and of course Plans (where to go next). Communication within the ICU team should be amicable and effective, with only one person speaking at a time. Bedside rounds are an occasion for all team members to express their opinion about a patient’s care or management so that a coherent plan can be formed. People should look forward to the rounds, be prepared and be happy to participate.
3. Have good leadership
A good leader is essential to build and support an effective team. A good leader needs to be open-minded, enthusiastic, supportive and pleasant, but not really a friend. A good leader should not avoid conflict but be able to recognise it early and act rapidly and fairly to resolve it and prevent escalation. A good leader is readily available and accessible to talk about any work-related subject, including errors or hard feelings. He/she should choose associates who are confident in their position and good team players. Being able to effectively delegate responsibility is important; doing everything oneself is not justifiable or sustainable and will make others feel inadequate. However, delegating does not mean abrogating all responsibility; the leader remains in overall charge of the team.
4. Include family members and close friends as part of the team
Relatives and close friends are often better placed than the ICU staff to identify problems such as delirium or behavioural changes. They can provide comfort and limit the need for restraints: it is so much better to feel the hand of your loved one on your arm! Visiting hours should be quite open as there is no reason to restrict them if everybody understands their rights and limitations. Relatives need to be happy with their relationship with the healthcare professionals looking after their loved one. This does not mean they are your friends and can do anything they want; family members must understand the rules. Make time to meet and talk with relatives; poor communication with family members can create bad feelings and conflict.
5. Discuss ethical decisions openly
End-of-life issues should be openly discussed and involve all team members, and the relatives and patient when possible. Making such difficult decisions using a consensus approach will help everyone feel more comfortable with the ultimate decision. Younger staff members must be encouraged to participate as this is an essential part of their training. Obviously, the autonomy of the patient should be respected whenever possible: remember principle number one above.
6. Discontinue interventions that are no longer needed
Once started, interventions are sometimes continued almost as routine, but the real necessity for any measure must be regularly reconsidered. Antibiotics should be stopped on time; catheters, endotracheal tube, and drains should be removed as soon as they are no longer needed. Even bed rest should be abandoned whenever possible. This does not mean that less is always better, just that the need for all interventions should be carefully and regularly re-evaluated. Feeding, ECMO, haemodynamic monitoring to guide cardiovascular support, blood transfusions, etc., must be given when needed, but not continued without good reason. The benefits must be repeatedly weighed against the risks for every intervention in every patient.
7. Use monitoring judiciously
As with interventions, the need for monitoring should be carefully considered and revised regularly. One should only monitor what needs to be monitored to ensure optimal care for that patient. Monitoring equipment can be frightening for the patient and their relatives and reduce patient mobility. It can also be distracting, with staff members focusing on the monitors rather than the patient. Some monitoring is, of course, required to ensure therapies are targeted appropriately for the individual patient - this is personalised medicine. For example, the use of fixed tidal volumes of 6 ml/kg of ideal body weight for all patients with acute respiratory failure, of X mL/kg of crystalloids over 1 or 3 hours in all patients with septic shock, or of vasopressors to target a mean arterial pressure of 65 mmHg in all patients is too simplistic as requirements can vary substantially from one patient to the other.
8. Minimise or avoid sedation as much as possible
Sedation is more often prescribed for staff comfort than for patient comfort, which is in direct opposition to the number one rule for patient wellbeing. The principle that patients who are treated with mechanical ventilation should be routinely sedated to ‘keep them comfortable’ (as is commonly argued) is incorrect. The same applies to patients in shock, ignoring the fact that these patients are typically obtunded and that all sedative agents have unwanted haemodynamic effects. The eCASH rule (Figure 2) should be applied, emphasising good pain control and replacing ‘comfort’ sedation with humanised care.
9. Encourage patients to mobilise
How many patients are out of bed or even out of their room in your ICU? Patients on mechanical ventilation and even on ECMO can be helped to move around, taking their machine with them. Even those who are bedridden can be taken outside (weather permitting). Importantly, all members of the team need to be persuaded that this approach is good for the patient, not only physically but also mentally - this is not something that should be forced. If the team members are not convinced of its value, the patients will not be encouraged to try either.
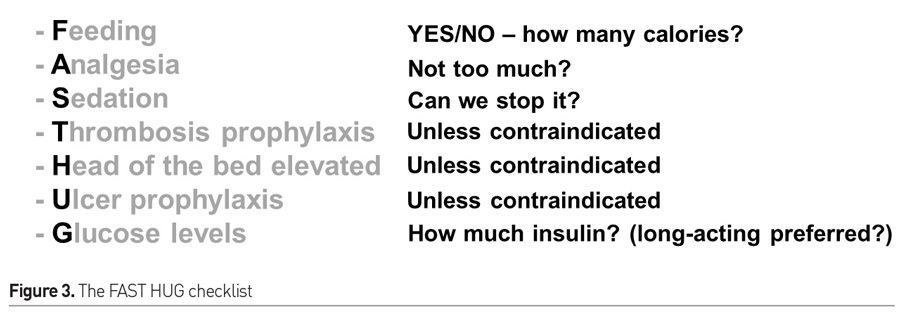
10. Don’t replace intelligent care with protocolised care
Protocols can be helpful to facilitate patient management. However, some variability in the care of the acutely ill is necessary as no two patients are identical. Excessive protocolisation may reduce the intellectual aspect of ICU care, the need and ability to reflect and adapt treatment to the individual. This effect may also limit the attractiveness of intensive care medicine to doctors and other healthcare practitioners, which could result in a vicious cycle, with fewer trained professionals leading to the use of more protocolised care to replace human input, resulting in the need for fewer staff members, and so on. Humans can sometimes forget important things, especially in the complex environment of the ICU, and simple checklists like the FAST HUG mnemonic can be useful for this purpose (Figure 3).
11. Ensure your ICU activities include the trio of clinical practice, teaching and research
Clinical practice is the most obvious aspect of critical care medicine and must be of high quality for patient and staff wellbeing. Quality of care must be audited regularly and if not good enough in one or more areas, plans put into action to improve it. Clinical teaching at the bedside is essential as it provides the optimal means of understanding the mechanisms of disease and the rationale for management in individual patients. Bedside teaching helps improve the knowledge of all the ICU team members, which will benefit current and future patients. Finally, clinical research must not be forgotten and is not limited to large university hospitals. Multicentre studies can involve all hospitals, and small studies can be conducted almost everywhere. Importantly, clinical research does not always lead to publications in major journals but is a way of helping people to be rigorous and to question a variety of aspects in the management of the critically ill. This can only be good for patient and staff wellbeing (Figure 4).
12. Smile!
I like to look at the faces of staff members when I enter an ICU for the first time. This is a good quality indicator: happiness at work creates motivation and a good atmosphere. People who feel good can provide better quality care with less stress. People should be happy to be at work to do their best to help others - this is the essence of critical care medicine.
Conflict of Interest
None.
