




ICU Management & Practice, Volume 17 - Issue 4, 2017
 PRINT OPTIMISED
PRINT OPTIMISED
A purchasing portfolio for more effective and efficient (medical) supply purchasing
This design study aims to develop a purchasing portfolio for a university hospital intensive care centre that enables the user to make strategic decisions about how to allocate scarce resources wisely across different purchase categories.
There
is a growing interest in the way hospitals purchase their (medical) products because
of increasing health system costs (Van Raaij 2016). The cost of medical
supplies is the second largest part of hospital budgets, after labour costs. By
purchasing more strategically, it is not only possible to decrease spending, but
also to increase the quality of products and the satisfaction of the staff
(Lichtenberger et al. 2010). The University Medical Center Utrecht (UMCU) wants
to increase its operational effectiveness (UMC Utrecht 2012) using multiple approaches,
including more strategic purchasing (UMC Utrecht 2013).
You might also like:Improving healthcare: the role of the human factors specialist
The aim of this design study is to develop a relevant, scientifically grounded tool, which enables the Intensive Care Center (ICC) of the UMCU to identify explicit purchasing strategies for their purchase categories by using a purchasing portfolio. The industrial sector often uses Kraljic’s (1983) purchasing portfolio as a foundation for decisions about strategic purchasing. The methodological guidelines of Van Aken and Andriessen (2011) form the foundation of this design study. Firstly, a review of the purchasing portfolio literature was performed to develop a theoretical framework. Next, semi-structured interviews with six experts were executed on two separate occasions; first, to diagnose the current situation, and later again to evaluate the tool that was designed as well as the results of a simulation of the tool. All experts work for the purchasing department of the hospital or have a management role in the ICC.
Purchasing accounts for approximately 30% of the total budget of a hospital and includes many different purchase categories, including advanced medical supplies but also office supplies (Lichtenberger et al. 2010). Professional purchasing can reduce the costs of products and/ or improve the quality of products (Schotanus and Telgen 2007; Lichtenberg et al. 2010; Miocevic 2011). Professional purchasing helps organizations to achieve their goals and improve their financial sustainability.
Purchasing portfolio model
Purchasing portfolio models acknowledge that not all purchase categories should be managed in the same way (Gelderman and Van Weele 2002). A purchasing portfolio model provides insight into which strategies can be used for which goods and services. It helps to make strategic choices (Gelderman and Van Weele 2002; Olsen and Ellram 1997), improve the profitability and achieve long-term goals of the organization (Coate 1983). The essence of a portfolio model is that there is a limited amount of resources (Coate 1983; Olsen and Ellram 1997). The use of a purchasing portfolio model leads to a differential approach in the balanced use of scarce resources (time, effort) for purchasing activities (Gelderman 2000).
In 1983 Kraljic introduced his purchasing portfolio model, leading to better insight into and management of supply risk and purchasing power. Power and dependence are very important in Kraljic’s model (Caniëls and Gelderman 2007). The dependence of the purchasing organization on a supplier is a power source for the supplier and vice versa (Caniëls and Gelderman 2005), resulting in an asymmetrical (power) relationship between buyer and supplier. The model was developed for manufacturing companies, but can easily be modified for service, government and nonprofit organizations (Olsen and Ellram 1997). The goal of our study was to find out which modifications of the Kraljic portfolio were needed to apply this model in the context of an intensive care centre. Developing a portfolio model starts with identifying factors that influence which strategy is most effective in which situation. Analysis and classification of the different factors is necessary (Fiocca 1982) to gain insight into the complexity and importance of these factors. Doing this in a team with different experts creates a shared vision on factors, strategies and purchasing effectiveness (Lichtenberger et al. 2010).
The first step in this design study was to analyse the current situation through observations and expert interviews. Over the years, the purchasing department of UMCU has increased its influence over the purchasing process, which has led to a better structured purchasing process (PP), resulting in more favourable purchasing conditions. In the past, purchasing was done by managers without specific purchasing training. A major step in the purchasing process is defining product specifications. This is done in a cross-functional (XF) team. Common factors for product specification include safety, quality, total costs, order volume, innovation, ease of use, switch possibilities and societal implications. Safety is an important factor for all respondents. The purchasing department ultimately buys the product.
More and more basic products are standardized across the hospital to capitalise on purchasing volume and achieve lower total costs. Standardisation leads to a more efficient PP where the ICC delegates the PP to the purchasing department. The management of the ICC can then focus on more important purchases. Suppliers try to influence the PP by contacting ICC managers directly by email, telephone and/or unannounced visits. Managers waste time on suppliers that sell standardized products. To stay innovative it is necessary to have contact with suppliers that have new products, but it is hard to differentiate between suppliers of strategic products and suppliers of standard products. Innovation is especially important for the ICC, because the patient population is very complex. This population demands special products that directly affect the quality of care for a specific patient or group of patients. To buy these complex products, expertise from the XF team is needed. Important factors for specifying these products are innovation, quality and switch possibilities. To make the right decision the XF team needs to have an intense relationship with the supplier resulting in long-term contracts, earlier available innovations and sometimes developing products together. Usually, this applies to just a few (strategic) suppliers and products. The supplier and the ICC share the objective to reach long-term goals. Besides supplier relationships, market strategy is a key factor determining what the most effective PP is. The market strategy depends on the number of suppliers that are able to deliver a product(group) resulting in a more efficient PP by obtaining some products as part of a bundle. To create power over the supplier it is vital to establish a large purchasing volume. Supplier relations and market strategies have a large impact on what type of PP is chosen for which purchase categories.
Purchase categories
In the second step of this study, insights from our review of the literature were combined with our analysis of the current situation to develop a classification of purchase categories. We created a decision tree, and by answering each of the four questions at every level with yes or no, products can be placed in a product class, as presented in Figure 1. Common factors have a major influence on the process of creating a purchasing portfolio. Based on these specifications, five product classes have been identified, all with their own specifications, strategies and consequences. Examples of products in each class are also provided in Figure 1.
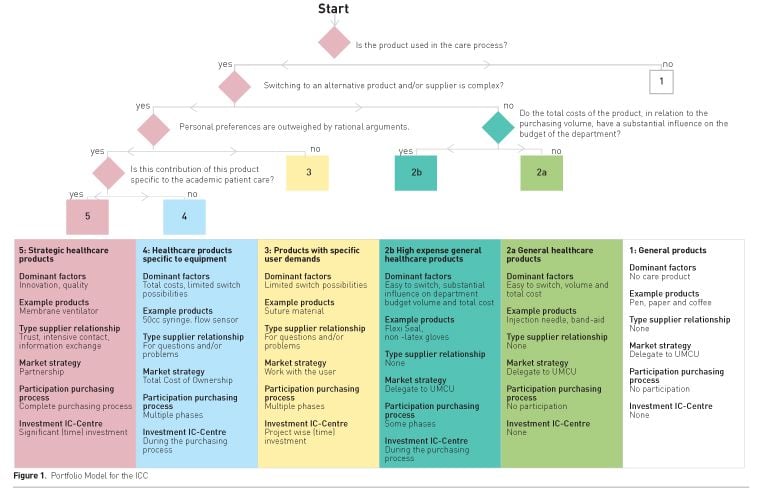
Figure 1. Portfolio Model for the ICC
General products
First of all, the ICC stocks and consumes general products not used in the care process. This product class asks for an efficient PP where product standardisation is optimised (Gelderman and Van Weele 2002; Olsen and Ellram 1997). The complete process has been delegated to the UMCU resulting in no effort from the ICC, lower prices and better purchasing contracts. ICC managers should not spend time on managing supplier relationships for these products.
General healthcare products
The second product class contains general healthcare products, which is split into subclasses 2a and 2b. Standardisation across the hospital is again important to increase purchasing volume (Gelderman and Van Weele 2002) and hence make these products easier to manage. The purchasing department uses the total volume to increase power over the supplier. It is in the interest of the ICC to standardise as many products as possible to achieve a significant decrease of the total costs (Olsen and Ellram 1997). These products are characterized by low switching costs. Only when the total costs of a product account for a significant part of the budget or when the product is important for the care process, will the ICC take part in the XF purchasing team resulting in some influence on the decisions. This distinguishes product classes 2a and 2b, with class 2a fully delegated to the purchasing department, and the ICC participating in the first phases of the PP for class 2b. Also for product class 2, ICC management should not spend precious time on managing supplier relationships.
Products with specific user demands
Class 3 consists of products with specific user demands. This makes switching products and/ or suppliers more difficult. The ICC needs to work with the user and the purchasing department to see if it is possible to switch to class 2 products resulting in lower total costs (Gelderman and Van Weele 2002). Class 3 products are generally hard to manage and require time and effort from ICC management to discuss standardisation potential with internal users (Olsen and Ellram 1997).
Care-related products (consumables)
Class 4 consists of care-related products (consumables) specific to equipment. It is vital to use the Total Cost of Ownership concept to make well-founded choices about equipment in combination with consumables. Most equipment is used for many years, and switching consumables is difficult or even impossible during the operational lifetime of the equipment. Significant time investment is necessary from ICC management, but only during the PP of the equipment. Furthermore, a regular review of consumables can be used to identify alternatives for consumables during the operational lifetime of the equipment.
Strategic healthcare products
Finally, class 5 consists of strategic healthcare products used for the specific patient population of an academic hospital. Care for these high-demand patients results in new scientific knowledge and innovative products can directly influence chances of survival. This makes this ICC different from an ICC in a non-academic hospital. In this product class the focus is on developing products for care together with the supplier. There is a long-term commitment, and creating a partnership with the supplier is essential (Olsen and Ellram 1997), with investments from both sides (Gadde and Snehota 2000). The ICC needs to be part of the complete PP to build the required buyer-supplier relationship and influence decisions.
ICC product portfolio
We
reviewed the current product portfolio of the ICC and classified them according
to our decision tree. This simulation of our portfolio model showed (see Figure 2)
that 75% of all products in stock at the ICC (classes 1 and 2a), can be managed
by fully delegating the PP to the purchasing department. Many suppliers from these
two product classes still demand an intense supplier relationship with the ICC,
according to the interviewees. This consumes time from ICC managers that is not
spent wisely. Significant time investment is needed in the first phases of the
PP for class 2b to keep control over a large part of the total costs. However,
these 58 products need to be purchased centrally by the UMCU to benefit from
larger volumes. A total of 21 products (class 3) need more attention to discuss
with internal users if switching is possible to be able to decrease the cost. A
rather large number of products (41 products) belong to product class 4,
representing consumables for which the ICC is locked in to specific suppliers. For
these products, ICC management needs to invest time whenever new equipment is
being considered. Only 8 products (class 5) require an intense supplier
relationship to benefit the specific population of the ICC. In this product class,
product volumes and costs for the organization appear lower due to research
funding– giving the supplier relationship an extra dimension. The interviewees
confirmed that the purchasing portfolio and the results from the simulation showed
various possibilities to improve the purchasing process for the ICC.
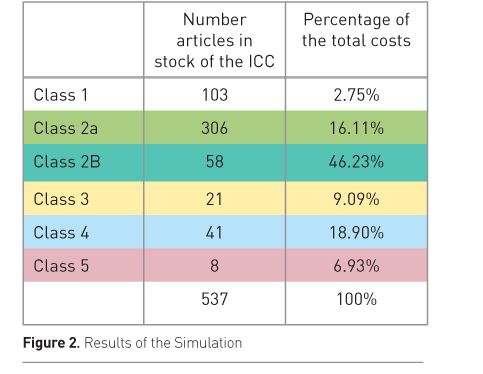
Figure 2. Results of the Simulation
Conclusion
The purchasing portfolio enables the ICC to easily classify a product and make conscious and strategic decisions about the allocation of scarce resources, such as time spent with suppliers. The portfolio can be applied at similar departments in (university) hospitals. Knowledge of purchasing portfolios like this one enables ICC managers to have meaningful discussions with purchasing professionals.
Funding
This
research did not receive any specific grant from funding agencies in the
public, commercial, or not-for-profit sector.
Abbreviations
ICC intensive care centre
PP purchasing process
XF cross-functional
References:
Caniëls MCJ, Gelderman CJ (2007) Power and interdependence in buyer supplier relationships: a purchasing portfolio approach. Industrial Marketing Management, 36(2), 219-29.
Coate MB (1983) Pitfalls in portfolio planning. Long Range Planning, 16(3): 47-56.
Fiocca R (1982) Account portfolio analysis for strategy development. Industrial Marketing Management, 11(1): 53-62.
Gadde LE, Snehota I (2000) Making the most of supplier relationships. Industrial Marketing Management, 29(4): 305-16.
Gelderman CJ (2000) Rethinking Kraljic: towards a purchasing portfolio model, based on mutual buyer–supplier dependence. Danish Purchasing & Logistics Forum, 27(10): 9-15.
Gelderman CJ, Van Weele AJ (2002) Strategic direction through purchasing portfolio management: a case study. Journal of Supply Chain Management, 38(1): 30-7.
Kraljic P (1983) Purchasing must become supply management. Harvard Business Review, Sept-Oct: 109-17.
Lichtenberger S, Everett N, Ungerman D (2010) How sourcing excellence can lower hospital costs. Health International, 10: 18-29.
Miocevic D (2011) Organizational buying effectiveness in supply chain context: conceptualization and empirical assessment. Journal of Purchasing & Supply Management, 17(4): 246-55.
Olsen R, Ellram L (1997) A portfolio approach to supplier relationships. Industrial Marketing Management, 26(2): 101-13.
Schotanus F, Telgen J (2007) Developing a typology of organisational forms of cooperative purchasing. Journal of Purchasing & Supply Management, 13(1): 53-68.
UMC Utrecht (2012) Begroting 2013. Via Vitaal, p. 1.
UMC Utrecht (2013) OPEX gaat UMC-breed verder. UMCkrant, p. 4.
Van Aken J, Andriessen D (2011) Handboek ontwerpgericht wetenschappelijk onderzoek [Handbook design-oriented scientific research]. Den Haag: Boom Lemma uitgevers.
Van Raaij E (2016) Purchasing value: purchasing and supply management’s contribution to health service performance, inaugural addresses Research in Management Series ref EIA-2016-068-LIS, Rotterdam: Erasmus Research Institute of Management.

