



HealthManagement, Volume 19 - Issue 2, 2019
 PRINT OPTIMISED
PRINT OPTIMISED
The foremost expert in critical care ultrasound on the value of natural vs artificial intelligence in medicine.
Ultrasound is a tool like no other in medicine. Most importantly, because it is a work of the hand and the eye, combining the art of reasoning, common sense (that is, intelligence), it provides a unique opportunity for the physician to be in direct contact with the patient.
Ultrasound is a tool like no other in medicine, not only because of its well-known qualities (non irradiating, repeatable etc). Most importantly, this is a work of the hand and the eye, combining the art of reasoning, the common sense (that is, intelligence), and a unique opportunity for the physician to be in direct contact with the patient. As to medicine, this is not a profession like any other. Ultrasound is therefore a genuine summit, a holy providence. The very interest of being an MD is to use one’s own intelligence, to put together all we have learned, for making decisions on the correct management of patients. Ultrasound is at the centre of many of these pathways.
So how about artificial intelligence (AI)? What has AI to do here? First note, this is an amusing oxymoron. Intelligence is the most sensitive, emotional expression of mankind. It allows human beings to survive from chaotic situations, also to make life more interesting, to practice art and so many wonderful achievements. Intelligence is fully linked with emotion, a miracle of life. Can such a holy gift be made artificial? I am not an expert in the field of AI, so I risk to go beyond my level of expertise, or to write trite remarks, but was kindly invited to submit my ideas. What I see is that people seem hypnotised by any new technology (not only AI), maybe for wanting to be like the others. Therefore, other people have the duty to be against, to just provide for a balanced world. I did this before as regards the previous trend, Internet, a revolution that brought unbelieavable advantages, allowing us to have everything immediately, but to the detriment of such disagreements that the overall result is only a slight progress of mankind, at the cost of an incredible energy. Now, we have to face all issues of Internet, which from occult, have become patent.
Regarding AI, the new trend in fashion, my two concerns are first to see it failing, generating comicotragical issues (this has begun, already); the second one is to see it not failing, winning over human intelligence. There would be nothing to admire, nothing worth applauding: I guess that a technology able to multiply the octets (mega, giga, tera...) will do things faster than standard human beings. Even if I find an authentic genius able to resist, we would just have to add one layer of technology (peta, exa, zetta if necessary), and the technology will eventually win. If not, we use a yotta level; or billions of yotta, etc. But which number will succeed to generate genuine emotion? The immense strength of emotion is that it does not require any artificial help, is the pure expression of intelligence. Intelligence is life. So what do we really want? To have things fast, or to live in an acceptable world with an acceptable life, with plenty of acceptable defaults?
Once we understand that the new technologies can do everything, their field of possibilities will no longer amaze us. This scenario will of course mean the end of all professions which require intelligence, that is, all interesting professions, all interesting lives. The argument advocating that AI will make the doctor (and other human beings) free of fastidious tasks seems to be a bit empty, and consequently, dangerous. To begin with, young students will cease to be interested in medical studies, and only robots (intelligent) will take care of us, all along our disease. We will not even thank anybody, it will be included in their programme (they can be formatted for recognising the word “thank you,” and answer what somebody decided to program, such as “just my duty,” or “do not forget to pay,” or “I am a simple robot, you know, I was programmed to listen to your emotion, but I have no human brain, sorry, you lose your energy).”
By the way, ultrasound is all the more unique, as it was “recently” rejuvenated, by being extended to critical ultrasound. I highlight the word “recently,” although I am proud to have built critical ultrasound since 1985 using a gray-scale 1982 technology (the ADR-4000®, visible now in museums). This technology was maybe antique, but the community forgot to exploit it correctly, that is, at the bedside. I am currently working on a Hitachi-405®, a gray-scale 1992 technology, slightly better (discontinued 9 years ago, not really replaced). Many doctors are persuaded that the recent revolution of ultrasound was the result of the miniaturisation (modern ultrasound machines look like laptops). While thinking so, these doctors avoid to give a medical name to this revolution, which is therefore attributed to the “technology.” This common belief is easily invalidated: ironically, our Hitachi-405® is smaller than all laptops in the only interesting dimension, the width. If we use our brain for a few seconds, the vertical dimension (small in laptops) is not a critical advantage in our hospitals, so far as our ceilings are always high enough. The real obstacles are lateral. In addition, laptop machines stay all the time embedded in their carts, and this is an excellent thing: a cart is a mandatory ergonomic part of critical ultrasound, within hospitals, the usual place for saving lives. A simple (natural) intelligence was sufficient for realising this. I, as a simple user, am fascinated by the blindness of the community regarding this detail. Building a new discipline using an old tool was my real pride, because it could generate a simple, elegant “revolution,” easy to implement, without destroying anything, without the need of a superhuman, artificial intelligence.
Critical ultrasound can be defined as a clinical science based on applications which were accessible but not used in the past. Lung ultrasound is the best example. Lung ultrasound (another oxymoron) was not supposed to exist. We spent however a lifetime (3 decades now) understanding the “ultrasound language” of the main vital organ. We mainly discovered its translational face: any physician dealing with the lung will find interest in lung ultrasound - including the specialists in medical imaging. Of use in its most dramatic application (cardiac arrest) or in routine (up to the family doctor), in seniors as well as babies, in rich or deprived patients, in healthy or scarse-resource countries, in protected settings (university hospitals) or isolated ones (from austere medicine to even spaceships), in any setting lung (and critical) ultrasound is used with no adaptation, this makes no real difference, this is one definition of holistic ultrasound.
Why is critical ultrasound a holistic discipline? This means, shortly, that its separated elements (the machine, the probe, the targets...) seem apparently unlinked, but their integration makes a homogeneous, synergic whole. As a single example, lung ultrasound allows echocardiography to be simplified (Lichtenstein 2014). As another example, I can perform a whole body critical ultrasound using one single probe. Our wide range microconvex probe has the perfect range and ergonomy for universal use in the critically ill. Most physicians who have learned to use critical ultrasound, especially lung ultrasound, have confided in me that they received a kind of accomplishment in their life. Their “previous” life was exciting but sometimes boring (too much paperwork), or too difficult with challenging settings. Our best acknowledgement is when some ladies (or opposedly) tell us that their husband (wife) comes home after work much more excited once they have discovered the art of critical and lung ultrasound. It sounds like a police investigation, nearly an endless game in many aspects.
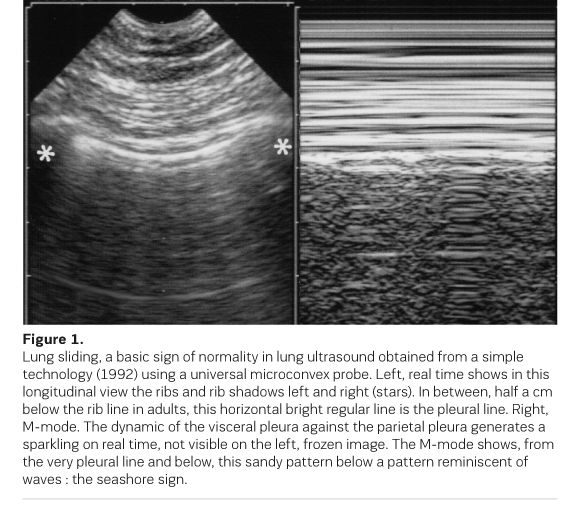
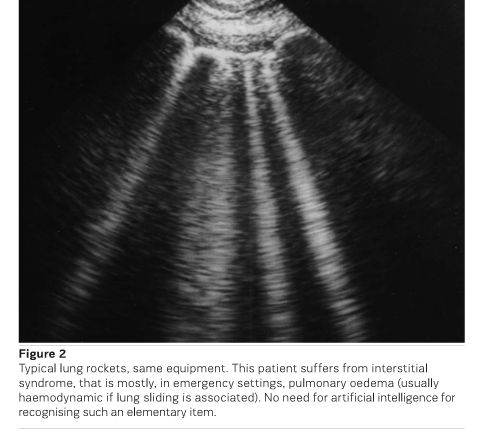
And now, we hear about AI in this field, such as automatic recognition of B-lines (among others). We shortly evoke some basis of lung ultrasound. Lung sliding is a parameter of prime importance (for diagnosing pneumothorax and inflammatory lung diseases), accessible to none of the modern technologies (Figure 1). The B-line is a comet-tail artifact, strictly defined according to seven criteria (Lichtenstein 2014). A certain concentration of B-lines, called lung rockets, defines interstitial syndrome (Figure 2). This sign has a critical relevance for promptly diagnosing numerous conditions: the diagnosis of pneumothorax; the diagnosis of pulmonary oedema (the analysis of lung sliding allowing to distinguish haemodynamic from inflammatory oedema, schematically). The indication for giving and discontinuing fluids in critically ill patients with circulatory failure (the FALLS-protocol), and many others. The search for pneumothorax is the first step of the SESAME-protocol, a focused critical whole body ultrasound approach used during a cardiac arrest. Our unit is always ready for it, so no time is lost (Lichtenstein and Malbrain 2015). When each second counts, we are not sure that AI will be accessible for showing the right way. For managing cardiac arrest, even if the SESAME-protocol can be done in a few seconds, years of exciting understanding are necessary, and this is precisely what keeps us so much attracted.
I want to remind that the (natural) intelligence is not a trait of exceptional people. Any human being is, by definition, intelligent. Many people think they are deprived of this gift, they just forget that the success is done by one third of it, but also one third of work, and... one third of luck. We can favour luck, we can work, even a lot. Intelligence is the only parameter where a direct action is useless. Suppressing the interest of intelligence would tempt people, we imagine, yet if (natural) intelligence is no longer necessary, we also imagine that, in a first step, then people will be happy (because of feeling favoured), and a minority will have to find a profession which does not require intelligence (if they succeed to find a job). Time passing, we don’t have the slightest idea of what such a “civilisation” would become. A life without the feeling to be useful, where AI will choose your partner (with perfect technical accuracy of course) scares us to a point that we begin to love the defaults of our life partner!
To conclude, even if ultrasound was long considered a technique in traditional imaging, in our field at least, critical ultrasound appears as a major help to the physician who has taken the best of physical examination for understanding the data appearing on the screen, helping to perform a visual medicine. All this occurs in a normal setting where the doctor remains a doctor (and the patient, a patient). That is, a deal between human beings first. That is a deal where natural intelligence and emotion work in symbiosis, that is, a genuine philosophy. Even in the age of AI, this strength will remain a priceless help. I foresee a bright future for ultrasound, this “sleeping giant” as many say recently, a genuine stethoscope according to our knowledge (Scopein, to see, and Stethos.... the chest wall).
Key Points
- AI, the new trend in fashion; two concerns are first to see it failing, generating comicotragical issues (this has begun, already); the second one is to see it not failing, winning over human intelligence
- The argument advocating that AI will make the doctor (and other human beings) free of fastidious tasks seems to be a bit empty, and consequently, dangerous
- I am proud to have built critical ultrasound since 1985 using a gray-scale 1982 technology (the ADR-4000®, visible now in some museums). This technology was maybe antique, but the community forgot to exploit it correctly, that is, at the bedside
- Building a new discipline using an old tool was my real pride, because it could generate a simple, elegant “revolution”, easy to implement, without destroying anything, without the need of a superhuman, artificial intelligence
- Critical ultrasound can be defined as a clinical science based on applications which were accessible but not used in the past
Next Article: AI applications in breast imaging
References:
Lichtenstein DA (2014) Lung Ultrasound in the Critically Ill - the BLUE-protocol. Springer-Verlag Ed, Heidelberg Berlin New York. Ann Intensive Care. 2014(4): 1. Available from: ncbi.nlm.nih.gov/pmc/articles/PMC3895677/
Lichtenstein DA, Malbrain ML (2015) Critical care ultrasound in cardiac arrest. Technological requirements for performing the SESAME-protocol - a holistic approach. Anaesthesiol Intensive Ther. 47(5): 471-81. Available from: ncbi.nlm.nih.gov/pubmed/26578398
