




ICU Management & Practice, ICU Volume 13 - Issue 2 - Summer 2013
A recent large prospective cohort study conducted on different types of surgery has demonstrated that the incidence of in-hospital mortality and postoperative pulmonary complications (PPCs)is relatively high. Moreover, PPCs are associated with prolonged hospital stay and higher hospital mortality (Pearse et al. 2012).Ongoing studies are trying to find effective strategies for improving outcome. A keystone in PPCs prevention and early treatment is intensive perioperative respiratory monitoring. In this review, the authors aim to describe different methods to monitor respiratory function during the perioperative period in general and under specific conditions, and the role of recently published predictive scores.
Respiratory Function during the Perioperative Period
The induction of anaesthesia and curarisation lead to a loss of normal coordination of respiratory muscles, reduction of diaphragmatic tone, decrease in functional residual capacity (FRC), oxygen reabsorption and changes in surfactant function. These factors are associated with the formation of atelectasis, collapse of small airways and decrease in respiratory system compliance. Atelectasis leads to deterioration of ventilation/perfusion ratio and increase of intrapulmonary shunt. Furthermore, the absence of positive end-expiratory pressure (PEEP), the use of high tidal volume ventilation and high plateau pressure (>10 ml/kg and >30 cmH2O, respectively) are associated with the occurrence of Acute Respiratory Distress Syndrome (ARDS) (Tusman et al. 2012). Pathogenesis of perioperativeARDS involves tidal recruitment and cyclic opening and closing of the boundary between aerated and collapsed lung units, and tidal over-distension in non-atelectasis lung units(Slinger 2008).
Basic Tools for Monitoring
Since early detection is essential for prevention and for delivery of appropriate treatment,such as non-invasive ventilation in atelectasis or adequate PEEP during general anaesthesia, in tegration of various monitoring tools is warranted.In a cohort of 2,000 reported incidents during general anaesthesia, simple pulse oximetry or capnography could detect over half of all events(Webb et al. 1993).
Pulse Oximetry
For prediction of PPCs, a large prospective cohort study in 2,464 patients undergoing surgical procedures by the ARISCAT group has shown that 28.6% of patients with SpO2≤ 90% developed at least one post-operative in-hospital pulmonary complication, therefore preoperative SpO2 has been included in the ARISCAT PPCs prediction score (Canet et al. 2010). In perioperative and recovery rooms, pulse oximetry plays a role in detection of hypoxaemia and related events, without affecting mortality (Moller et al. 1993; Pedersen et al. 2009).A recent study showed that pulse oximetry surveillance reduced rescue events and intensive care unit transfers( Taenzer et al. 2010).
Since SpO2 is physiologically related to PaO2, according to the oxyhaemoglobin dissociation curve, in patients with PaO2 higher than 60 mmHg, SpO2 has low sensitivity for detection of hypoxemia. However a study inARDS patients has demonstrated a good correlation between SpO2/FiO2 ratio and PaO2/FiO2 ratio and proposed its use in substitution of PaO2/FiO2 ratio (Rice et al. 2007).
In the emergency room pulse oximetry can underestimate oxygenation in patients with septicaemia and septic shock (Wilson et al. 2010). Nail polish, especially white, black, purple and dark blue can affect the measurement of SpO2 although the range of error is ±2% (Hinkelbein et al. 2007).
Capnography
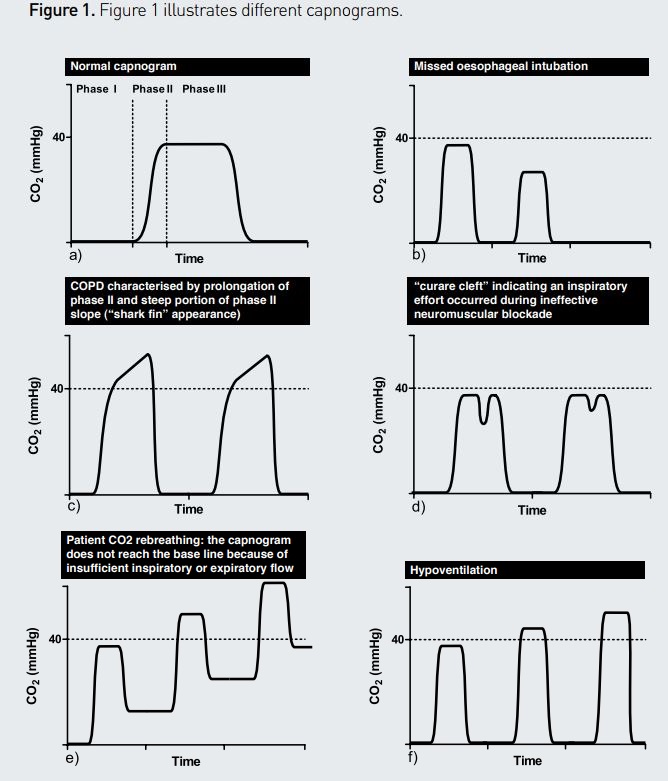
The capnogram is a simple non-invasive method for the assessment of blood CO2, and can reflect alveolar ventilation, pulmonary perfusion and appropriate connection of ventilatory apparatus to the patient.The waveform characteristics of capnography comprise three phases(see Figure 1). Phase I, which is breathed out initially, represents the dead space due to airway anatomy and apparatus. Phase II represents the alveolar gas emptying from alveoli. Phase III represents CO2 removal from alveolar gas.The end-tidal CO2 concentration (PetCO2) is measured at the highest point in phase III.This parameter is an indirect measurement of PaCO2. Figure 1 also shows common pathological findings in capnography.
Other Tools
Current evidence supports the potential role of protective low tidal volume ventilation in healthy lungs during general anaesthesia in decreasing the incidence of PPCs(Pelosi et al. 2011; Moriondo et al.2012; SerpaNeto et al.2012;Hemmes et al. 2013).The role of PEEP level isstill controversial. However, data from large randomised controlled trials should be available soon (Hemmes et al. 2011).Ongoing large prospective observational and randomised controlled studies will provide further information (University Hospital, Clermont-Ferrand ;Hemmes et al. 2013).
Respiratory Mechanics
In the intraoperative period, the airway pressure and compliance measurement could be helpful to optimise the appropriate tidal volume, plateau pressure and PEEP. In some circumstances, such as postoperative intra-abdominal surgery, obesity and patients with increased intra-abdominal pressure (IAP),respiratory compliance is not only affected by lungs but also by the chest wall, and the airway pressure might not represent the real stress and-strain of the lungs. Preoperative oesophageal catheter placement can measure transpulmonary pressure (Ptp), work of breathing and intrinsic PEEP in high-risk patients. Ptp is the distending force of the lung and is the difference between Palv and Ppl where Palv is the alveolar pressure and Ppl is the intrapleural pressure, measured by balloon placement in the oesophagus.Thus, the measurement of oesophageal pressure could be of help for better titration and optimisation of the pressure required for alveolar recruitment, the tidal volume, and safe plateau pressure as well as the PEEP level during the perioperative period (Pelosi et al. 2011). Furthermore, oesophageal pressure monitoring can be used in the post-operative period to minimise patient-ventilator asynchronies, particularly in COPD patients.
Haemodynamics and Respiration
The emergence of new mini-invasive techniques for haemodynamic assessment allows continuous monitoring of cardiac output and other parameters at the bedside, giving prompt information about the role of haemodynamics in the development of respiratory failure. Many of these methods are based on pulse pattern analysis, which can be measured even on a peripheral arterial line, during or after major surgery (Jones et al. 2006; Cannesson et al. 2009). Recently a totally non-invasive alternative has been proposed, but its accuracy is under debate (Broch et al. 2013). Minimally invasive techniques allow transpulmonary thermodilution to estimate extravascular lung water (EVLW) and EVLW index (EVLWi) (Michard 2007).Transthoracic echocardiography has been proposed for estimation of cardiac output (Demirkol et al. 2013).The abovementioned techniques allow the evaluation of stroke volume variation, which is of emerging interest in the evaluation of patient fluid responsiveness (Cannesson et al. 2009).
Most studies conclude that haemodynamic goal-directed therapy can improve outcome in high-risk surgical patients(Vincent et al. 2012), especially in terms of reduction of post-operative complications, while mortality reduction is significant only in very high-risk surgical patients (Cecconi et al. 2013).
Ultrasonography and Respiration
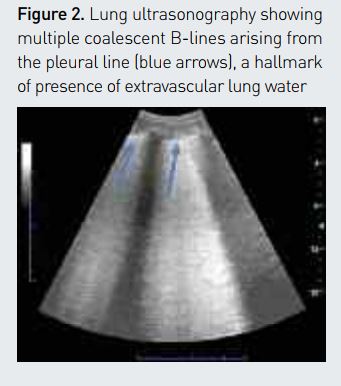
There is emerging consensus about the possibility of using bedside lung ultrasound (LUS) for respiratory monitoring (Bellani et al. 2012; Luecke et al. 2012;Via et al. 2012), for the early assessment of PPCs such as pneumothorax (Ueda et al. 2011), and to monitor the response to non-invasive ventilation (Liteplo et al. 2010) and pharmacological therapy (Via et al. 2010). LUS is capable of estimating EVLW non-invasively at the bedside (Baldi et al. 2013) (see Figure 2). Computer-aided quantification of LUS has been recently proposed (Corradi et al. 2013), and could lead to a reduction in time-consumption and operator-dependence.
Monitoring in Specific Conditions
Obesity, Obstructive Sleep Apnoea
In morbid obesity the forced vital capacity, maximal voluntary ventilation and expiratory reserve volume are markedly reduced. During anaesthesia, an increase in BMI has a good correlation with a decrease in lung volume, lung compliance and oxygenation (Pelosi et al. 1998) and with increase of lung resistance. The decrease of functional residual capacity is linked with atelectasis formation.(Pelosi et al. 2010). Ventilator settings during anaesthesia in obesity should include: 1) low tidal volume ventilation 2) open lung approach by PEEP and recruitment manoeuvre 3) FiO2 less than 0.8 (Pelosi et al. 2010).We recommend monitoring carefully airway plateau pressure, intrinsic PEEP and Ptp. Further studies are warranted to define the optimal respiratory monitoring and setting in this group of patients.
In patients with obstructive sleep apnoea undergoing elective surgery, an oxygen de-saturation index ≥ 5 is associated with higher incidence of PPCs (Hwang et al. 2008). Thus, in patients with high sleep apnoea clinical scores should be closely monitored for oxygenation during the perioperative period (Gali et al. 2009). In a recent large cohort study determining the impact of sleep-disordered breathing (SDB) on postoperative outcome in patients undergoing elective surgery, despite an association of SDB with postoperative cardiopulmonary complications, the diagnosis of SDB was not independently associated with increased in-hospital mortality (Mokhlesi et al. 2013).
Role of Recently Published Predictive Scores
Risk factors associated with PPCs depend on basic underlying status, method of anaesthesia, smoking status, type of surgery and post operative anaesthetic drugs. The type of surgeries most closely associated with PPCs are abdominal aortic aneurism repair, oesophagectomy and major abdominal surgery (22.5, 18.9 and 14.2% respectively) (Smetana et al. 2006). Several investigators demonstrated that the overall risk of PPCs can be predicted, and developed different scores. Most of the parameters needed for score calculation can be assessed at the bedside, and these scores can help physicians to identify high-risk patients who require intensive monitoring (see Table 1).
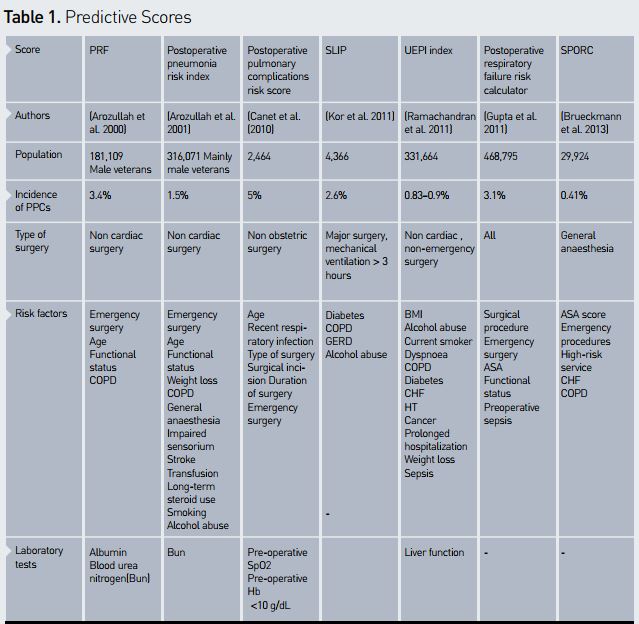
Investigators from the Veterans Health Administration combined several factors to develop a postoperative respiratory failure risk index (PRF) and pneumonia risk index, already validated, for postoperative respiratory failure in major non-cardiac surgery based on National Surgical Quality Improvement Program (NSQIP) data. These indexes have some limitations in terms of generalisability because the majority of the population were male veterans(Arozullah et al. 2000;Arozullah et al. 2001), and the inclusion of numerous risk factors in the index makes it difficult to use in everyday clinical practice. These indexes were included in a systematic review (Smetana and Lawrence 2006) and in the 2006 American College of Physicians guideline (Qaseem et al. 2006).
Canet et al., for the ARISCAT group, have recently identified variables, namely pre-operative arterial oxygen saturation, pre-operative haemoglobin concentration (less than 10 g/dL) and respiratory infection in the previous month, as strong predictors. Additionally, the study has confirmed that surgical procedure and duration are predictors of PPCs. The areas under ROC curve are 90 and 80 for the development of PPCs predictive index and the validation of this index, respectively. The promising advantages of this score are simple clinical assessment and use of objective variables. A large European study (PERISCOPE) has been completed, and will act as external validation of this score (Canet et al.2011).
Kor et al. developed the surgical lung injury prediction score (the SLIP score) for distinguishing patients undergoing high-risk surgery WHO will need mechanical ventilation during general anaesthesia for longer than three hours and for predicting the occurrence of postoperative ARDS. This score can identify patients that will develop early postoperative ARDS with anAUC of 0.82 (95% CI 0.78-0.86) (Kor et al. 2011).However, this study could be biased by its single centre retrospective design and heterogeneity of population.
Based on ACS-NSQIP data, on 222,094 patients, Ramachandran et al. developed the unanticipated early postoperative intubation risk class index (UEPI index), suggesting that close respiratory monitoring during non-invasive ventilation after abdominal surgery might reduce tracheal intubation in high risk patients (Ramachandran et al. 2011). Additionally, Gupta et al. developed the postoperative respiratory failure (PRF) risk calculator based on a logistic regression model. PRF risk calculator is available online and as a mobile application designed for physicians (Gupta et al. 2011). Bruekmann et al. reported the Score for Prediction of Postoperative Respiratory Complications (SPORC), focusing on the early re-intubation within three days after surgery as primary endpoint, with an AUC of 0.81 that can be easily used preoperatively by anaesthesiologists (Brueckmann et al. 2013).
Conclusion
Respiratory monitoring is essential in the perioperative period to optimise mechanical ventilation, for risk stratification and for early detection of postoperative pulmonary complications. A deep knowledge of different monitoring techniques is crucial to improve the quality of care in surgical patients.
References:
ArozullahAM, Daley J et al.(2000) Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery. The National Veterans Administration Surgical Quality Improvement Program. Ann Surg, 232(2):242-53.
ArozullahAM, Khuri SF et al.(2001) Development and validation of a multifactorial risk index for predicting postoperative pneumonia after major non-cardiac surgery. Ann Intern Med, 135(10):847-57.
Baldi G, Gargani Let al.(2013) Lung water assessment by lung ultrasonography in intensive care: a pilot study. Intensive Care Med, 39(1):74-84.
Bellani G, MauriT et al.(2012) Imaging in acute lung injury and acute respiratory distress syndrome. Curr Opin Crit Care, 18(1):29-34.
Broch O, Bein B et al.(2013)A comparison of continuous non-invasive arterial pressure with invasive radial and femoral pressure in patients undergoing cardiac surgery. MinervaAnestesiol, 79(3):248-56.
Brueckmann B,Villa-Uribe JL et al.(2013) development and validation of a score for prediction of postoperative respiratory complications. Anesthesiology, 118(6):1276-85.
Canet J, Gallart L et al.(2010) Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology, 113(6):1338-50.
Canet J,Hardman J et al.(2011) PERISCOPE study: predicting post-operative pulmonary complications in Europe. Eur JAnaesthesiol, 28(6):459-461.
Cannesson M, Musard H et al.(2009)The ability of stroke volume variations obtained withVigileo/FloTrac system to monitor fluid responsiveness in mechanically ventilated patients. AnesthAnalg, 108(2): 513-7.
Cecconi M, Corredor C et al.(2013) Clinical review: Goal-directed therapy what is the evidence in surgical patients? The effect on different risk groups. Crit Care, 17(2):209.
Corradi F, Ball L et al.(2013)Assessment of extravascular lung water by quantitative ultrasound and CT in isolated bovine lung. Respir Physiol Neurobiol, 187(3):244-9.
Demirkol S, Balta Set al.(2013) Can trans-thoracic echocardiography be used as a reference method for cardiac output measurement? Minerva Anestesiol, 79(5):571.
Gali B,Whalen FX et al.(2009) Identification of patients at risk for postoperative respiratory complications using a preoperative obstructive sleep apnea screening tool and post-anesthesia care assessment . Anesthesiology, 110(4):869-77.
Gupta H, Gupta PK et al.(2011) Development and validation of a risk calculator predicting postoperative respiratory failure. Chest, 140(5):1207-15.
Hemmes SN,Abreu MG et al.(2013) ESA ClinicalTrials Network 2012: LAS VEGAS - local assessment of ventilatory management during general anaesthesia for surgery and its effects on postoperative pulmonary complications: A prospective, observational, international, multicentre cohort study. Eur JAnaesthesiol, 30(5):205-7.
Hemmes SN, Serpa NetoA et al.(2013) Intraoperative ventilatory strategies to prevent postoperative pulmonary complications: a meta-analysis. Curr OpinAnaesthesiol, 26(2):126-133.
Hemmes SN, Severgnini P et al.(2011) Rationale and study design of PROVHILO - a worldwide multicenter randomized controlled trial on protective ventilation during general anesthesia for open abdominal surgery. Trials, 12:111.
Hinkelbein J, Genzwuerker HV et al.(2007) Effect of nail polish on oxygen saturation determined by pulse oximetry in critically ill patients. Resuscitation, 72(1):82-91.
Hwang D, Shakir N et al.(2008)Association of sleep-disordered breathing with postoperative complications. Chest, 133(5):1128-34.
Jones D, Story D et al.(2006) Perioperative pulse contour cardiac output analysis in a patient with severe cardiac dysfunction. Anaesth Intensive Care, 34(1):97-101.
Kor DJ,Warner DO,AlsaraA, Fernández-Pérez ER, Malinchoc M, Kashyap R, Li G, Gajic O (2013) Derivation and diagnostic accuracy of the surgical lung injury prediction model.Anesthesiology, 115(1):117-28.
LiteploAS, MurrayAF et al.(2010) Real-time resolution of sonographic Blines in a patient with pulmonary edema on continuous positive airway pressure.Am J Emerg Med, 28(4): 541 e5-8.
LueckeT, Corradi F et al.(2012) Lung imaging for titration of mechanical ventilation. Curr OpinAnaesthesiol, 25(2):131-40.
Michard F (2007) Bedside assessment of extravascular lung water by dilution methods: temptations and pitfalls. Crit Care Med, 35(4):1186-92.
Mokhlesi B,Hovda MD et al.(2013) Sleep-disordered breathing and postoperative outcomes after elective surgery: analysis of the Nationwide Inpatient Sample. Chest, Mar 28 [Epub ahead of print]
Moller JT, Johannessen NW et al.(1993) Randomized evaluation of pulse oximetry in 20,802 patients: II. Perioperative events and postoperative complications. Anesthesiology, 78(3):445-53.
MoriondoA, Marcozzi Cet al.(2012) Impact of mechanical ventilation and fluid load on pulmonary glycosaminoglycans. Respir Physiol Neurobiol, 181(3):308-20.
Pearse RM, Moreno RP et al.(2012) Mortality after surgery in Europe: a 7 day cohort study. Lancet, 380(9847):1059-65.
PedersenT, MollerAM et al.(2009) Pulse oximetry for perioperative monitoring. Cochrane Database Syst Rev,(4): CD002013.
Pelosi P, Croci M et al.(1998)The effects of body mass on lung volumes, respiratory mechanics, and gas exchange during general anesthesia.Anesth Analg, 87(3):654-60.
Pelosi P, Gregoretti C (2010) Perioperative management of obese patients. Best Pract Res ClinAnaesthesiol, 24(2):211-25.
Pelosi P, LueckeT et al.(2011) Chest wall mechanics and abdominal pressure during general anaesthesia in normal and obese individuals and in acute lung injury. Curr Opin Crit Care, 17(1):72-9.
Pelosi P, Rocco PR(2011)Ventilator-induced lung injury in healthy and diseased lungs: better to prevent than cure! Anesthesiology, 115(5):923-5.
QaseemA, SnowV, Fitterman N,Hornbake ER, LawrenceVA, Smetana GW, Weiss K,Owens DK, Aronson M, Barry P, Casey DE Jr, Cross JT Jr, Fitterman N, Sherif KD,Weiss KB; Clinical Efficacy Assessment Subcommittee of the American College of Physicians.(2006) Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing non-cardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med, 18;144(8):575-80.
Ramachandran S.K,Nafiu OO et al.(2011) Independent predictors and outcomes of unanticipated early postoperative tracheal intubation after non-emergent, non-cardiac surgery. Anesthesiology, 115(1): 44-53.
RiceTW, WheelerAP et al.(2007) Comparison of the SpO2/FiO2 ratio and the PaO2/FiO2 ratio in patients with acute lung injury or ARDS. Chest, 132(2):410-7.
Serpa NetoA, Cardoso SO et al.(2012)Association between use of lung protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta analysis. JAMA, 308(16):1651-9.
Slinger P (2008) Perioperative lung injury. Best Pract Res Clin Anaesthesiol, 22(1):177-91.
Smetana GW, LawrenceVA et al.(2006) Preoperative pulmonary risk stratification for non-cardiothoracic surgery: systematic review for theAmerican College of Physicians. Ann Intern Med, 144(8):581-95.
TaenzerAH, Pyke JB et al.(2010) Impact of pulse oximetry surveillance on rescue events and intensive care unit transfers: a before-and-after concurrence study. Anesthesiology, 112(2):282-7.
Tusman G, Bohm SH et al.(2012)Atelectasis and perioperative pulmonary complications in high-risk patients. Curr Opin Anaesthesiol, 25(1):1-10.
Ueda K,AhmedW et al.(2011) Intraoperative pneumothorax identified with trans-thoracic ultrasound. Anesthesiology, 115(3):653-5.
University Hospital, Clermont-Ferrand. Intraoperative protective ventilation in abdominal surgery (IMPROVE study) In: ClinicalTrials.gov [Internet]. Bethesda (MD):National Library of Medicine (US). 2000- [cited 2013 JUNE 12].Available from: http://clinicaltrials.gov/show/NCT01282996.
Via G, Lichtenstein D et al.(2010)Whole lung lavage: a unique model for ultrasound assessment of lung aeration changes. Intensive Care Med, 36(6):999-1007.
Via G, Storti E et al.(2012) Lung ultrasound in the ICU: from diagnostic instrument to respiratory monitoring tool. Minerva Anestesiol, 78(11):1282-96.
Vincent JL, Fagnoul D (2012) Do we need to monitor cardiac output during major surgery? Anesthesiology. 117(6):1151-2.
Webb RK, van derWalt JH et al.(1993)The Australian Incident Monitoring Study.Which monitor?An analysis of 2000 incident reports. Anaesth Intensive Care, 21(5):529-42.
Wilson BJ, Cowan HJ et al.(2010)The accuracy of pulse oximetry in emergency department patients with severe sepsis and septic shock: a retrospective cohort study. BMC Emerg Med, 10:9.


