



HealthManagement, Volume 19 - Issue 1, 2019
 PRINT OPTIMISED
PRINT OPTIMISED
Incentivising patients with tokenomics of health data
A cryptocurrency that represents the value of health information can motivate individuals to make their health data shareable to those who are willing to pay for it.
Tokens are well established in the context of
Blockchain technology and cryptocurrencies.
It’s a digital asset that has a utility or a
payment function. Very often, it’s a hybrid token and
possesses both properties. However, technically, it
is just a piece of cryptographic code of no intrinsic
value. Although Blockchain and its related cryptocurrencies
are a recent development, tokens have been
the subject of psychological research for a long time.
In psychology, tokens are used to shape a target
behavior, and therefore tokens have to be backed by
reinforcers. A relation between a token of no intrinsic
value with an unconditioned reinforcer like food or
a conditioned one like money has to be established
by reinforcement. The law of effect (Thorndike 1898) describes that behaviour which is followed
by pleasant consequences as having a higher likelihood
of being repeated, whereas unpleasant consequences
decrease the likelihood of repeat behaviour.
The effectiveness of a token reward as a means of
behaviour modification has not only been observed
in humans but also in primates (Wolfe 1936) or
pigeons and rats (Skinner 1948; Skinner 1953). In humans,
it is often applied in cognitive behavioral therapy
and childrearing.
But how does that apply to health data and how
could the tokenisation of health data be the solution
of some of the most pressing problems in modern
healthcare?
Health data as the currency of healthcare systems
Modern healthcare runs on data. Everybody is on
the hunt for data in order to optimise processes or develop better therapies. Tremendous amounts of
data are being generated by medical documentation,
regulatory requirements, and patient care (Raghupathi 2010). In addition, precision medicine and the
general trend of digitisation in healthcare lead to a
constant rise of data being gathered at the individual
user or patient’s level (Andreu-Perez et al, 2015;
HM Government UK 2014). Another driving force in
this massive growth of data is the individual himself
when using a fitness or wellness app.
There are only estimates what personal health
data are worth, but it can be deducted from what
companies are willing to invest in order to gather
those data. IBM bought Truven Health Analytics for
$2.6 billion to train Watson on 200 million patient
records, meaning that one record was worth 13 USD.
It is a low price if you take into account what pharmaceutical
companies invest in order to gather clinical
trial data and real-world evidence. Prices that
are being paid for so-called post-market surveillance
might be a good indicator of the data value, with an
average of €441 per patient paid to the physician
providing the data (Spelsberg et al 2017).
It is needless to say, that in today’s data economy, wherever there is a value generated out of data, it
is not the individual as a data provider who profits
directly from the monetisation of its data. It results
in a lack of incentives for individuals to demand or
record, digitise, and update their health data. Hence,
it perpetuates the current system of monopolisation
of health data leading to siloes and inefficiencies
instead of motivating the individual being in
control of his data.
Tokens as incentives to digitise health data
Most people are only interested in their health data
when they are sick or when somebody they know is
suffering from a health problem, but there are ways
to motivate them to tend to their health data. In a
recent survey in Switzerland, 43% of all people said
they would be willing to provide their personal data
to medical research, either for free or for a reduction
of their health insurance premium (Tagesanzeiger 2017). In comparison, 54% of internet users are
willing to share their health data with their health
insurance, if they receive incentives such as vouchers
or premium reduction (Statista 2015). However, 79%
of German online users want the power to decide
who can access their health data (BKK Dachverband
Gesundheitsreport 2016). It shows that healthcare
systems must incentivise individuals to take control
over their data. At the same time a technical infrastructure
is needed, where everybody who seeks data can ask individuals for their consent to make
their health data shareable.
A decentralised marketplace to tokenise health data
Blockchain technology can facilitate such an infrastructure
in the form of a decentralised marketplace
where the access to health data is under the control
of the individual.
Information seekers can post their query and individuals
can remain anonymous and decide whether
or not they want to share their data. With the tokens
in a Blockchain-based marketplace, a reward can be
automatically transferred on the basis of a digital
contract once the data has been delivered. Such a
system has a clear advantage over a fiat currencybased
system where always a middleman has to be
involved and the large population of unbanked individuals
cannot participate.
In Figure 1 the token economy of the Health
Information Traceability platform is presented. A
payment and utility token facilitates transactions
of health information. Information seekers acquire
tokens to incentivise individuals to digitise and share
their data, while individuals can: a) redeem bonuses/
services that are offered by service providers on the
platform; b) trade it for another cryptocurrency; or c)
exchange it for cash at designated exchanges. Individuals
can also monetise their data that is stored in external repositories and share revenues with the
information holders such as personal health records,
claims processing companies, hospitals and pharmacies.
The central asset to be exchanged in the
HIT-ecosystem is information that has a token value
attached to it. The token value depends on how
much the network participant values the information
in question.
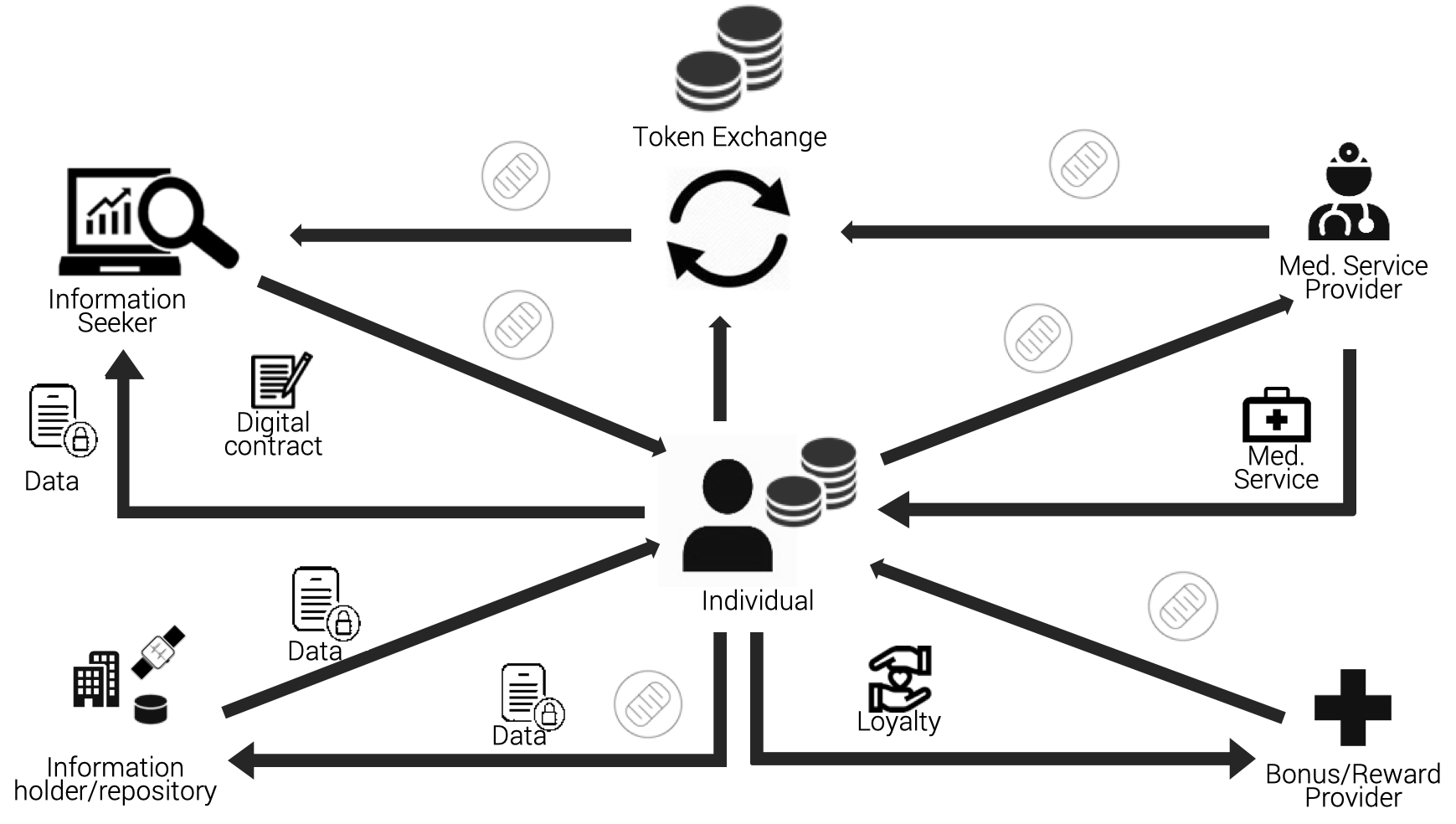 Figure 1. HIT Token economy (HIT Foundation 2018)
Figure 1. HIT Token economy (HIT Foundation 2018)Use cases for tokenising health information
• Research
Researchers have direct access to potential
study participants
• Population health data
Population survey and representative surveys
can be conducted via contacting individuals
directly
• Compliance Support
Individuals receive tokens when predefined health goals that are incorporated in a digital
contract are achieved.
Solutions with Blockchain-enabled ecosystem
Such a distributed ecosystem can be implemented
with Blockchain technology, making transaction
processes transparent and more efficient at the
same time. A Blockchain-based token system is
predestined to align incentives among ecosystem
participants, for example, providers of health information
and those who want to analyse health data.
It allows the latter to have direct access to providers
of health information without the need for intermediaries.
At the same time, it puts individuals in
control of the use and monetisation of their health
data. Tokenisation of health data motivates individuals
to make their data shareable, thus solving
the fundamental problem of modern healthcare.
Key points
- Healthcare runs on huge volumes of data
- Value of health data varies
- Patients can be financially-incentivised to control their health data
- Blockchain technology can facilitate establishment of decentralised data marketplace
References:
BKK Dachverband Gesundheitsreport 2016. Splendid Research.
HIT Foundation (2018) Whitepaper. Available from: hit.foundation/documents/Personalised Health and Care 2020, Framework for Action.
National Information Board HM Government UK (2014) Available from gov.uk/government/uploads/system/
uploads/attachment_data/file/384650/NIB_Report.pdf
Raghupathi W (2010) Data Mining in HealthCare. In Healthcare Informatics: Improving Efficiency and Productivity. Edited by Kudyba S. Taylor & Francis 211– 223.
Skinner, BF (1948) 'Superstition' in the pigeon. Journal of Experimental Psychology 38, 168-172.
Skinner, BF (1953) Science and human behavior. SimonandSchuster.
Spelsberg A, Prugger C., Doshi P, Ostrowski K., Witte T, Hüsgen D et al. (2017) Contributi on of industry funded postmarketing studies to drug safety: survey of notifications submit ed to regulatory agencies. BMJ 356:j 337
Statista (2015). Gesundheitsdateneine Fragedes Preises. Available from de.statista.com/infografik/3822/eebermittlung-elektronischer-gesundheitsdaten-fuer-verguenstigungen/
Tagesanzei ger (2017) So käuflichsind wir. Available from mobile2. tagesanzeiger.ch/articles/599ac823ab5c37
455e000001
Thorndike, EL (1898) Animal intelligence: An experimental study of the associative processes in animals.
Psychological Monographs: General and Applied, 2(4),i-109.
Wolfe, JB (1936) Effecti veness of token rewards for chimpanzees. Comparative Psychological Monographs 12, 1–72.
