HealthManagement, Volume 18 - Issue 5, 2018
 PRINT OPTIMISED
PRINT OPTIMISED
Basic components of effective performance improvement programmes include patient safety, process improvement, customer service, professional staff assessment, and education, each of which requires strategies for implementing continuous programmes to monitor performance, analyse data, implement change, and meet regulatory requirements.
To improve the safety and quality of the care that radiologists provide, and to allow radiologists and radiology personnel to remain competitive in an increasingly complex environment, it is essential that all imaging departments establish and maintain managed, comprehensive, and effective performance improvement programmes. Although the structure and focus of these programmes can vary, a number of common components exist, many of which are now widely mandated by organisations that regulate the field of radiology. Basic components include patient safety, process improvement, customer service, professional staff assessment, and education, each of which requires strategies for implementing continuous programmes to monitor performance, analyse data, implement change, and meet regulatory requirements.
You might also like: Quality and Safety In Radiology
The field of quality management, including performance improvement and patient safety, is characterised by a host of confusing and overlapping terminologies. In essence, a variety of processes can be introduced to monitor quality (quality control) and safety (risk management) under a departmental umbrella (quality assurance) that serves as a cog in the larger institutional culture of safety (total quality management). The ultimate goal is to continuously improve the effectiveness of what we do (performance improvement) (Kruskal et al. 2009).
Who are the customers?
It is important to know precisely who your customers are and to understand their opinions of your services. One approach is to identify who your customers are, determine their needs and expectations, and then meet and continuously try to exceed these expectations (Adams 1994).
Four major categories must be known when evaluating customer satisfaction (Alderson 2000):
- the factors on which customers base their evaluations of the quality of service
- how to identify your customers
- how to measure your customers’ satisfaction levels
- how to balance in practice interpersonal and technologic skills.
A process described by Reinertsen et al. (2007) illustrates how improved patient outcome relates to improved efficiency and reduced time wastage. In their system, messages and messengers should be carefully chosen, physician involvement should be visible, trust should be built within each quality initiative, and communication should be candid and open. However challenging such a process may be, an essential goal should be to demonstrate the positive benefits of participation.
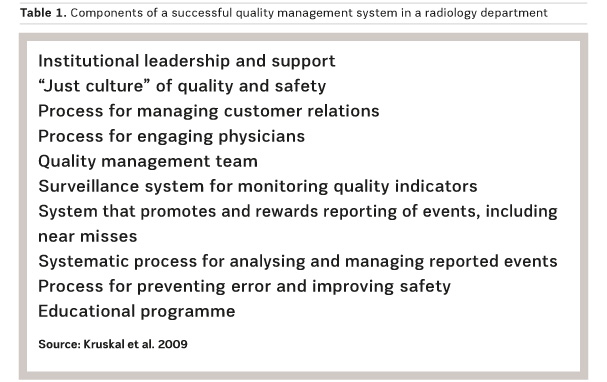
Components of a successful quality management system in a radiology department
The structure and components of a departmental performance improvement programme vary depending on the size of the department and hospital, the nature of the practice and the services offered, and the institutional mission and culture of quality and safety. Examples of ingredients that we consider essential to the implementation of a successful quality management enterprise in a radiology department are shown in Table 1. Other important elements include a focus on the customer and the processes, an understanding of process variation, a willingness to experiment with implementation of ideas, and teamwork (Applegate 2004). Quality and safety processes fall into five major categories: patient safety, process improvement, customer relations, assessment of physician performance, and education (“SICPE”). Many components overlap; for example, a system for communicating abnormal results falls under process improvement, patient safety, physician assessment, and customer relations (Kruskal et al. 2009).
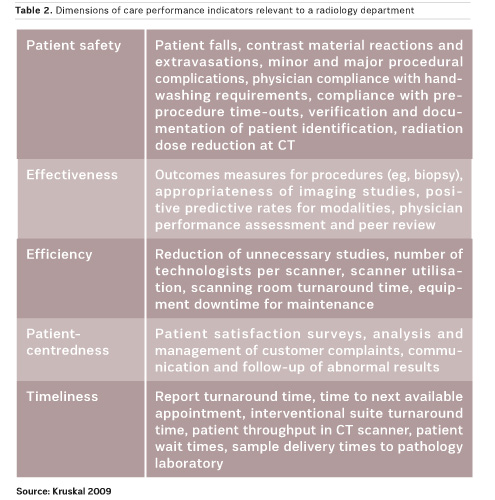
Dimensions of care
The use of quality management indicators, particularly customer satisfaction surveys, is not a fully standardised and established process in many radiology departments (Ondategui-Parra 2004). In radiology, the identity of the customer is not clear. Is it the patient, the referring physician, or the in-house referring department? All customers should be assessed for their satisfaction levels. Many hospitals are trying to align their stated missions with the dimensions of care highlighted in the Institute of Medicine report Crossing the quality chasm (Committee on Quality of Health Care in America 2001), which states that patient care should be safe, effective, efficient, patient-centred, and timely—categories that are readily applicable to the field of radiology (Table 2).
Quality management indicators
Because imaging services are widely used and affect patient care in every area of hospital, much attention has been focused on quality assurance in radiology departments over the past several years (Hillman 2006; Khorasani 2009; Johnson 2009; Steele 2009). However, measuring the quality of imaging services is inherently difficult, and scientifically sound metrics are lacking. Moreover, the review of patient records to document the effect of diagnostic imaging on the care outcome is costly in staff time and labour.
In 2001, the Institute of Medicine published the report Crossing the quality chasm, which specified six goals for healthcare quality improvement efforts: that healthcare be safe, effective, patient-centred, timely, efficient, and equitable (Committee on Quality of Health Care in America 2001). Given the growing demands for quality improvement in radiology practice, it is increasingly important to develop a standard set of metrics for the routine evaluation of radiology department operations and patient care. Such metrics also could be used in conjunction with the Practice Quality Improvement programme (part of the American Board of Radiology maintenance of certification process) to measure individual radiologists’ performance (Khorasani 2009).
The departmental mission, vision and values must be articulated by the leadership in the formulation of four categories of measurement: patient safety and quality of care, stakeholder management (management of the interests of internal and external stakeholders), operations management (management of core operations and enabling functions), and financial management. These four categories, which were inspired by the Kaplan-Norton balanced scorecard, represent key strategic principles of the department and broadly aim to:
a) accommodate all aspects of department performance
b) provide a common baseline for communicating results interdepartmentally within the institution and to external organisations
Within each of these four categories, key performance indicators (KPIs) must be formulated to align with one of the key strategic principles. Next, one or more specific metrics must be defined to allow measurement of each KPI (Hani et al. 2010).
Radiology-specific KPIs
The definition of radiology-specific KPIs should be a collaborative effort of the radiology department and the hospital administration. Hospital administrators are most knowledgeable about the institution’s strategic direction, and the success of the radiology department depends on the alignment of its KPIs with the institutional strategy. Priority should be given to the KPIs that are considered by both the hospital and the radiology department to align most closely with the institutional strategy and vision. The costs of measuring those parameters should be shared between the radiology department and the hospital. The hospital can allocate existing resources and personnel to help the radiology department collect and analyse the data, and radiologists can volunteer their time (Hani et al. 2010).
Conclusion
Healthcare services have a distinct position among other services due to the highly involved and risky nature of services and the general lack of expertise possessed by consumers. This makes conceptualising and measuring service quality in healthcare settings more important and at the same time more complex.
All radiological departments are expected to establish and maintain effective quality, safety and performance improvement programmes. Essential components of such programmes include adherence to the basic principles of quality management and appropriate utilisation of quality tools.
Quality improvement is not a passive process, it requires a careful, dedicated and continuously planned effort by a number of skilled and committed team members, with the aim to do the right thing in a timely fashion in every case. This process can be sustained by offering rewards and celebrating successes, with all lessons learned disseminated throughout the department or organisation.
Key Points
- One approach is to identify who your customers are, determine their needs and expectations, and then meet and continuously try to exceed these expectations
- Patient care should be safe, effective, efficient, patient-centred, and timely, categories that are readily applicable to the field of radiology
- Radiology-specific KPIs should be a collaborative effort of the radiology department and the hospital administration
References:
Abujudeh HH et al. (2010) Key performance indicators for measuring and improving radiology department performance. Radiographics 30(3): 571-80.
Adams HG, Arora S (1994) Total quality in radiology: a guide to implementation. Boca Raton, FL: St Lucie Press; CRC Press.
Alderson PO (2000) Noninterpretive skills for radiology residents: customer service and satisfaction in radiology. AJR Am J Roentgenol 175: 319–23.
Applegate KE (2004) Continuous quality improvement for radiologists. Acad Radiol 11: 155–61.
Committee on Quality of Health Care in America, Institute of Medicine (2001) Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy Press. Available from nap.edu/catalog/10027/crossing-the-quality-chasm-a-new-health-system-for-the
Hillman BJ (2006) Quality begins at home. J Am Coll Radiol 3(12): 899–900.
Johnson CD et al. (2009) Quality initiatives: developing a radiology quality and safety program: a primer. RadioGraphics 29(4): 951–9.
Khorasani R (2009) Objective quality metrics and personal dashboards for quality improvement. J Am Coll Radiol 6(8): 549–50.
Kruskal JB et al. (2009) Strategies for establishing a comprehensive quality and performance improvement program in a radiology department. Radiographics 29(2): 315-29.
Ondategui-Parra S et al. (2004) Practice management performance indicators in academic radiology departments. Radiology 233: 716–22.
Reinertsen JL et al. (2007) Engaging physicians in a shared quality agenda. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement. Available from ihi.org/resources/Pages/IHIWhitePapers/EngagingPhysiciansWhitePaper.aspx
Steele JR, Schomer DF (2009) Continuous quality improvement programs provide new opportunities to drive value innovation initiatives in hospital-based radiology practices. J Am Coll Radiol 6(7): 491–9.

