




Emergency physicians can safely reduce x-rays in children with injured ankles by as much as 23 percent, resulting in cost and time savings for patients, according to Canadian researchers who conducted a cost analysis of the Low Risk Ankle Rule (LRAR). The findings are reported in the journal Annals of Emergency Medicine.
"Currently, x-rays are ordered for up to 95 percent of children who come to emergency departments with ankle injuries, though only 12 percent of those x-rays show fractures," says the study's lead author Kathy Boutis, MD, MSc, of The Hospital for Sick Children and the University of Toronto in Toronto, Canada. "Widespread implementation of the LRAR could lead to a safe reduction of x-rays in children with ankle injuries, reducing unnecessary radiation exposure and healthcare costs."
Dr. Boutis and her colleagues compared children (aged 3 to 6 years) with ankle injuries at emergency departments that did and did not implement the LRAR. At emergency departments using the LRAR to assess children with acute ankle injuries, there were 22.9 percent fewer ankle x-rays and healthcare costs were $36.93 less compared with those that did not use the rule.
Despite the reduction in x-rays, the researchers found no significant differences in the frequency of missed clinically important fractures or in use of healthcare resources after a patient was discharged from the emergency department.
"Our findings are good news for the two million American and Canadian children with hurt ankles who visit emergency departments each year: although most currently receive x-rays, many do not actually need them," Dr. Boutis points out.
She also cites potential cost savings. For example, a publicly funded healthcare system's use of the LRAR to decide if x-rays are necessary in children with ankle injuries has modestly reduced health system costs -- without increasing patient costs. "In a privately funded healthcare system like the one in the Unites States, the cost savings would likely be realised by the patient or insurer," says Dr. Boutis.
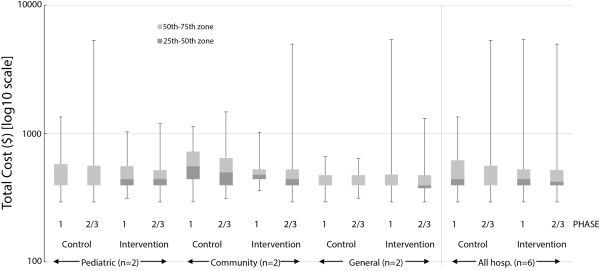
Figure 1. Effect of the Low Risk Ankle Rule on total costs at hospital-specific intervention versus control sites. All values are in Canadian dollars. Paediatric=paediatric ED located in tertiary care children's hospitals. General=general ED located in urban university-affiliated teaching hospitals. Community=community ED located in suburban hospitals with a limited teaching or academic mandate.
Source and image credit: American College of Emergency Physicians
"Currently, x-rays are ordered for up to 95 percent of children who come to emergency departments with ankle injuries, though only 12 percent of those x-rays show fractures," says the study's lead author Kathy Boutis, MD, MSc, of The Hospital for Sick Children and the University of Toronto in Toronto, Canada. "Widespread implementation of the LRAR could lead to a safe reduction of x-rays in children with ankle injuries, reducing unnecessary radiation exposure and healthcare costs."
Dr. Boutis and her colleagues compared children (aged 3 to 6 years) with ankle injuries at emergency departments that did and did not implement the LRAR. At emergency departments using the LRAR to assess children with acute ankle injuries, there were 22.9 percent fewer ankle x-rays and healthcare costs were $36.93 less compared with those that did not use the rule.
Despite the reduction in x-rays, the researchers found no significant differences in the frequency of missed clinically important fractures or in use of healthcare resources after a patient was discharged from the emergency department.
"Our findings are good news for the two million American and Canadian children with hurt ankles who visit emergency departments each year: although most currently receive x-rays, many do not actually need them," Dr. Boutis points out.
She also cites potential cost savings. For example, a publicly funded healthcare system's use of the LRAR to decide if x-rays are necessary in children with ankle injuries has modestly reduced health system costs -- without increasing patient costs. "In a privately funded healthcare system like the one in the Unites States, the cost savings would likely be realised by the patient or insurer," says Dr. Boutis.
Figure 1. Effect of the Low Risk Ankle Rule on total costs at hospital-specific intervention versus control sites. All values are in Canadian dollars. Paediatric=paediatric ED located in tertiary care children's hospitals. General=general ED located in urban university-affiliated teaching hospitals. Community=community ED located in suburban hospitals with a limited teaching or academic mandate.
Source and image credit: American College of Emergency Physicians
References:
Boutis K et al. (2015) Cost Consequence Analysis of Implementing the Low Risk Ankle Rule in Emergency Departments. Annals of Emergency Medicine,
July 14, 2015; DOI:
http://dx.doi.org/10.1016/j.annemergmed.2015.05.027
Latest Articles
healthmanagement, radiation, ankle injury, fractures, x-rays, emergency department
Emergency physicians can safely reduce x-rays in children with injured ankles by as much as 23 percent, resulting in cost and time savings for patients, according to Canadian researchers.



