




ICU Management & Practice, Volume 23 - Issue 1, 2023
 PRINT OPTIMISED
PRINT OPTIMISED
Based on the concepts and the checklist criteria for an ideal sepsis biomarker presented in the article Sepsis Diagnosis: Clinical signs, Scores, and Biomarkers in this issue of ICU Management & Practice, we update and review the potential use of Pancreatic Stone Protein (PSP) in adults, children, and neonates.
Pancreatic Stone Protein in Adults
First described in the 1970s, this protein was only evaluated as a potential biomarker in sepsis in 2000 (Graf 2020). Since then, laboratory, animal, and clinical studies have accumulated on the Pancreatic Stone Protein (PSP), with over 600 studies now published. A recent review collecting 14 studies and 2161 patients suggested PSP was an early biomarker of sepsis (Eggimann et al. 2019), confirmed by a second systematic review with 23 studies in 3191 patients (Fidalgo et al. 2022), including a prospective multicentre study (Pugin et al. 2021) and a meta-analysis (Prazak et al. 2021). PSP is a 16 kDa C-type lectin protein mostly produced by the pancreas and the intestine and is believed to play a role as a damage-associated molecular pattern (DAMP). PSP has been used to diagnose and characterise sepsis even in severe inflammatory states without infection, such as in trauma patients (Keel et al. 2009; Klein et al. 2020), postoperative patients (Klein et al. 2020) such as post-cardiac surgery patients (Klein et al. 2015), severely burned patients (Klein et al. 2021a), and in ARDS (Klein et al. 2021b).
Diagnosis of infection and sepsis with PSP in adults
A meta-analysis (Prazak et al. 2021) suggests that PSP is more sensitive and specific (ROC AUC 0.81 – 95%CI 0.78-0.85 – SE 0.017) than CRP (ROC AUC 0.77 – 95%CI 0.73-0.80 – SE 0.019) and PCT (ROC AUC 0.78 – 95%CI 0.74-0.82 – SE 0.022) to diagnose infection. The combination of CRP with PSP further enhances its accuracy (ROC AUC 0.90 – 95%CI 0.87-0.92), with higher sensitivity 0.81 (0.77-0.85) and specificity 0.84 (0.79-0.90) for discriminating infection from non-infection compared to other biomarkers or combination of biomarkers.
In a multicentre study (Pugin et al. 2021), the diagnostic accuracy of PSP (AUC 0.75 – 95%CI 0.67-0.82), CRP (AUC 0.77 – 95%CI 0.69-0.84) and PCT (AUC 0.75 – 95%CI 0.68-0.82) for sepsis were similar, but the combination of CRP plus PSP had the best accuracy (AUC 0.79 – 95%IC 0.72-0.86).
In this latter study, the cut-off of PSP to detect infection was lower than that for sepsis (Prazak et al. 2021). Until 2020, PSP levels were determined using an ELISA technique. Since 2020, PSP could be accurately measured using the rapid (<10 minutes), point-of-care abioSCOPE® diagnostic platform using a nanofluidic technology (CE certified 2020) and the PSP-abioKIT® (In Vitro Diagnostic Regulation IVDR 2022, Instruction fur use IFU = the risk of sepsis, Abionic, Epalinges, Switzerland). The measurement of PSP levels became very robust and accurate using this novel nanofluidic precision technique coupled with highly specific antibodies with high affinity. A correlation between the PSP levels measured by ELISA and the abioSCOPE® can be found and used to compare PSP studies before and after 2020 (abioSCOPE® ng/ml = 4.6 x ELISA ng/ml + 30 ng/ml - 95%IC 0.39-0.59) (Benningo et al. 2022). In healthy subjects, PSP measured using the PSP-abioKIT® is under 44 ng/ml (median 42 ng/ml, 5-95% percentiles 27-61 ng/ml, lowest/highest 23-74 ng/ml). In patients without infection or sepsis but with co-morbidities, PSP is under 88 ng/ml. The PSP cut-off for the diagnosis of infection in the meta-analysis was 233.3 ng/ml (44.2 ng/ml multiplied by 4.6 + 30 ng/ml) and 290.5 ng/ml for sepsis in the multicentric study. This 290.5 ng/ml value gave the best AUC in the ROC (0.75; 0.67 - 0.82) to differentiate patients with and without sepsis. Interestingly in this study, all patients with sepsis had PSP values > 300 ng/ml already three days before sepsis and > 450 ng/ml on the day of sepsis, compared to the non-sepsis group who had PSP values under 200 ng/ml. A study including 357 patients with infection or sepsis managed in outpatient clinics showed that PSP measured using the PSP-abioKIT® performed at home can differentiate patients with confirmed bacterial infection (median PSP 131 ng/ml, IQR 83-205) from those with sepsis (PSP 156 ng/ml, 90-286), p=0.016 (Loots et al. 2022). For CRP and PCT, the value for infection was CRP 58 mg/L (20-117) and 85 mg/L (34-141), respectively, for sepsis (p<0.001) and for infection PCT 0.08 ng/ml (0.03-0.21) and 0.26 ng/ml (0.1-1.4) respectively (p<0.001). Unfortunately, the absence of a control group without infection did not allow to determine the negative predictive value nor PSP cut-offs as support for antibiotic therapy initiation. In a study performed in the emergency room in 156 patients with suspicion of sepsis, the PSP measured using the PSP-abioKIT® was used to differentiate patients without infection or uncomplicated infections from patients with sepsis. Combining patient age (< 50 years old) with PSP (excluding COVID-19 patients), the PPV is 100% and NPV 84.4% for PSP < 199 ng/ml. In the 13 false negative patients (5 COVID-19 patients, six immunocompromised patients), there were only four patients with bacteraemia (with CRP > 100 mg/ml), and then finally, four false negatives out of 156 patients, i.e., the NPV could be of 96.7%. PSP < 90.5 ng/ml (PSP-abioKIT®) and CRP < 136.5 mg/l have been shown to have a 99% NPV for mortality in patients admitted to the emergency department for SARS-CoV2 infection (Van Singer et al. 2021). At the time of sepsis or septic shock in severe COVID-19 patients, the mean PSP was 275.4 ± 190.3 ng/ml (SD) and 320.9 ng/ml ± 155.7 ng/ml, respectively (Ventura 2021).
Potential use of combining CRP and PSP
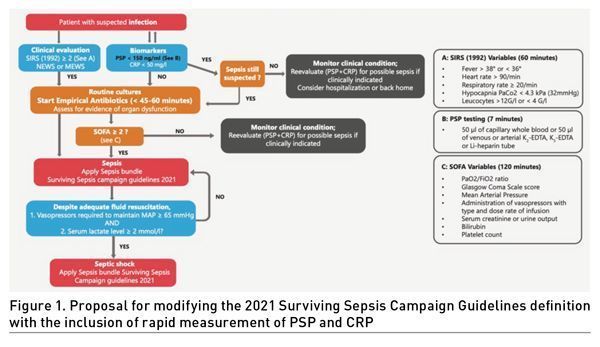
As recently proposed, PSP may be integrated into the definition of sepsis in a severely burned patient (Niggemann et al. 2021).In view of the clinical results summarised above, PSP, as well as the combination of PSP plus CRP, we propose that they could be added to the 2021 SSC guidelines (Evans et al. 2021). They have the potential to increase the rapid diagnosis accuracy of bacterial infection and sepsis and help to start antibiotics as soon as possible, within 45 to 60 minutes. They also may prove very useful to rule out the diagnosis of sepsis based on good NPV and prevent unnecessary broad-spectrum antibiotic therapy (Figure 1). PSP levels < 150 ng/ml are associated with a very good NPV and allow reasonably to decide not to start antibiotics, particularly when combined with a plasma CRP value < 50 mg/l. We recommend starting antibiotics and following the 2021 SSC guidelines for values above these cut-offs. However, clinical evaluation remains the priority in therapeutic choices. At the time of admission, very high PSP values (> 397 ng/ml ELISA = 1,856 ng/ml PSP-abioKIT® and > 346 ng/ml ELISA = 1,621 ng/ml) predict mortality (Que et al. 2012; Que et al. 2015). However, the abioSCOPE® does not currently measure PSP values > 600 ng/ml (PSP-abioKIT®).
Pre-symptomatic diagnosis of nosocomial sepsis in adults
PSP increases as early as 48 to 72 hours before the development of clinical signs of nosocomial sepsis, certainly in relation to preclinical steps of the dysregulated response of the body to bacterial infection: systemic inflammation response and/or dysregulated organ response. This occurs before the elevation of CRP and PCT. This was the result of a prospective study in a homogeneous population of 90 severely burned patients requiring ICU management (Klein et al. 2021a). The authors concluded, "Irrespective of the sepsis definition, PSP was the only marker to demonstrate a highly significant interaction between time and group (sepsis versus no sepsis) (p < 0.001) with a 3.3-5.5-fold increase within 72 hrs. before the event of sepsis, whereas CRP, PCT, and WBC showed only mild undulations”. A prospective multicentre study including 243 severely ill patients (Pugin et al. 2021) concluded: “Serial PSP measurement demonstrated an increase of this marker the days preceding the onset of signs necessary to clinical diagnose sepsis” (Figure 2). This study confirms that prospective daily measurement of PSP may be used for pre-symptomatic diagnosis of nosocomial sepsis. The NPV of PSP (PSP-abioKIT®) is 91.6% at D-3 sepsis with a cut-off at 152 ng/ml, 92.5% at D-2 sepsis with a cut-off at 173 ng/ml, 91.1% at D-1 sepsis with a cut-off at 175 ng/ml, 89.6% at sepsis with a cut-off at 194 ng/ml (Pugin et al. 2021). A study performed in 128 patients with severe COVID-19 requiring ICU management and mechanical ventilation showed PSP levels < 150 ng/ml in those without sepsis or septic shock, while CRP and PCT values < 180 mg/l and < 0.5 ng/ml, respectively (Ventura 2021). In the control group without sepsis (n=51), the daily variation of PSP was only 4.5 ng/ml (-11.3 to 20.4, p=0.574), demonstrating the stability of this biomarker in the absence of an event. For the 39 patients who developed sepsis, PSP increased from 184 ng/ml at D-4 to 275.4 ng/ml on the day of sepsis, with a statistically significant increase from D-2 to D0 (p=0.015 and p=0.007). The CRP remained high during these four days, around 200 mg/l, and the PCT increased only since D-2 but in a non-significant manner (p=0.24 and 0.30). For the 33 septic shocks, PSP was already above 300 ng/ml in the three days preceding the event without much variation over these three days, and at the time of septic shock, PSP reached 320.9 ng/ml (SD 155.7 ng/ml), CRP 213.7 mg/l (SD 88.4 mg/l), and PCT 1.24 (SD 1.44 ng/ml). Based on the available data in ICU patients, it is proposed not to initiate antibiotic therapy for suspected nosocomial sepsis if PSP levels (PSP-abioKIT®) are < 200 ng/ml. It also seems safe not to perform additional blood or radiological tests. It can also be proposed to start empirical broad-spectrum antibiotic therapy if PSP levels are > 300 ng/ml. If the PSP is in the grey zone between 200 and 300 ng/ml, this corresponds to a zone of moderate risk of sepsis, and the decision to initiate further investigations and to treat with antibiotics is left to the clinician in charge (Figure 2a and 2b).

Figure 2a: Pre-symptomatic diagnosis of nosocomial sepsis. Daily routine PSP monitoring of nosocomial sepsis.
 Figure 2b: Daily PSP evaluation
Figure 2b: Daily PSP evaluation
Limitations of Pancreatic Stone Protein use in adults
PSP is mostly produced by the pancreas and is significantly higher at baseline in patients with diabetes mellitus compared to non-diabetics (Klein et al. 2015), but its increase allows the diagnosis of sepsis in diabetic patients. Obesity (BMI >30 kg/m2) did not influence PSP levels. PSP levels were significantly higher in elderly patients above the median age of 67 years. The difference in PSP among diabetic patients lost statistical significance after adjusting for age.
Not surprisingly, PSP is elevated in acute pancreatitis and cannot be used to diagnose sepsis in those patients. PSP has, however, been shown to predict outcomes (AUC 0.841) and mortality in these patients (Rodríguez Rojas et al. 2021). In chronic renal failure, the baseline PSP value is significantly higher than in healthy subjects, but PSP can be used to diagnose sepsis in this situation (Satomura et al. 1995). According to an unpublished analysis of a prospective multicentre study data (Pugin et al. 2021), there is no linear correlation between PSP and renal function as assessed by creatinine values. A prospective clinical study is underway to analyse the usefulness of PSP in patients with AKI and the effect of renal replacement therapy.
Pancreatic Stone Protein PSP in Children
In children, there are currently ten studies published, including one for values in healthy children of different age groups (Schlapbach et al. 2015), three for neonatal sepsis (Rass et al. 2016; Schlapbach et al. 2013); Wu R et al. 2017), and six for sepsis in children (Wu Q et al. 2017; Jiří et al. 2014; Peng et al. 2015; Huo et al. 2017; Cui et al. 2017; Saleh et al. 2023). These studies were all performed using the ELISA technique. Several studies are underway with the PSP-abioKIT® for neonatal and children sepsis.
PSP values in healthy children and adults
In 372 healthy subjects, the authors reported, “PSP circulating levels were not gender-dependent and ranged from 1.0 to 99.4 ng/ml with a median of 9.2 ng/ml. PSP increased significantly between the age categories, from a median of 2.6 ng/ml in very preterm newborns to 6.3 ng/ml in term newborns, to 16.1 ng/ml in older children (p < 0.001)" (Schlapbach et al. 2015).
PSP in neonatal sepsis
In 2013, PSP levels were measured in 137 infants with a gestational age of > 34 weeks admitted with suspected early-onset sepsis (Schlapbach et al. 2013). A bio-score combining PSP and PCT was the best predictor of EOS (0.83; 95 % CI 0.74–0.93; p<0.001) and resulted in a NPV of 100% and a PPV of 71%. In 2016, a hospital-based prospective study on 104 neonates showed a 96.2% sensitivity, an 88.5% specificity, and a 95.8% PPV to diagnose sepsis for an AUC of 0.87 (Rass et al. 2016). The authors concluded, "The high negative predictive value of PSP (89.3%) indicates that the serum PSP level is a good marker for diagnosis of early onset neonatal sepsis and can be used to limit hospital stay and antibiotic use in neonates treated for suspected sepsis". In 2017, a study of 119 neonates admitted with suspected sepsis showed significantly higher PSP levels in the infected group compared to the control group at all time points (p<0.001) (Wu R et al. 2017).
PSP in the diagnosis of infection and sepsis in children
In 2014, a prospective observational study evaluated 61 children (0-19 years old) with SIRS or sepsis over a five-day evaluation period (Jiří et al. 2014). PSP levels were significantly higher in patients with a PELOD score of 12 or higher or those with MODS. Patients who died tended to have higher PSP levels. In 2017, a study compared 187 children with suspected acute osteomyelitis with 80 healthy control children (Cui et al. 2017). Serum levels of PCT and PSP were higher in children with acute osteomyelitis than those non-infected (p<0.01). The AUC values of PCT and PSP were 0.77 (95% CI, 0.70–0.83) and 0.80 (95% CI, 0.73–0.86), respectively. The AUC value of the combination of PCT plus PSP reached 0.90 (95% CI: 0.85–0.94). In 2017, a prospective case-control study (Peng et al. 2015) included 159 children with sepsis and 20 without sepsis. On day 1 after PICU admission, PSP levels in the sepsis and severe sepsis groups were significantly higher than in the control group. In 2023, a study including 180 septic children and 100 control shows that PSP has a significant diagnostic value in evaluating critically ill patients with sepsis and detecting sepsis severity (Saleh et al. 2022). The same study shows that PSP had the capacity to discriminate non-survivors from survivors.
PSP for prognosis of sepsis in children
In 2017, a study included214 children developing nosocomial sepsis (Wu Q et al. 2017). The AUC of combined PCT, high sensitivity (hs)-CRP, and PSP was 0.92 (95% CI, 0.87–0.95), which was significantly increased compared with PCT, hs-CRP, or PSP alone (p<0.001). Multivariate logistic regression revealed that PCT, hs-CRP, and PSP correlated independently with the prognosis of children with sepsis (p<0.001). In 2017, 106 hospitalised children with sepsis were enrolled (Huo et al. 2017). The multivariate logistic regression also showed that PTC, hs-CRP and PSP were independent predictors of death in patients with sepsis (p<0.001).
There are currently no published studies on the routine, daily use of PSP for pre-symptomatic diagnosis of nosocomial sepsis in neonates and children.
Agenda for Further Research
An economic study published in 2022 in Health Economic Review (Schneider et al. 2022) shows that measuring PSP (US$ 52 per test) in adults at admission reduces costs by US$ 1,688 per septic patient in the emergency department and US$ 3,315 per septic patient in the ICU compared to standard of care. The national saving in the US could be up to US$ 7 billion per year. In January 2023, more than 20 prospective and interventional studies on PSP in various settings, including to guide antibiotic de-escalation, are underway.
Conclusion
Sepsis remains a major public health problem, defined as suspected bacterial infection together with a dysregulated host response and organ dysfunction. Early diagnosis and management are susceptible to decreasing both sepsis-associated morbidity and mortality. Early diagnosis is currently based only on sensitive but non-specific clinical signs combined with clinical scores. In adults and children, the combination of CRP with PSP, allows high accuracy in the early diagnosis of infection and sepsis, with a potentially sufficiently high NPV (above 90%, even higher in neonates) to rule out infection and sepsis.
PSP increases at least 48 to 72 hours in adults before clinical signs of sepsis, allowing pre-symptomatic diagnosis of nosocomial sepsis. The good negative predictive value of the PSP could demonstrate its usefulness in the decision not to start antibiotic therapy or not to perform complementary exams and help solve the major public health problem of antimicrobial-resistant bacteria in hospitals and ICUs. Measuring PSP in adults at admission reduce costs per septic patient in the ED in the ICU compared to the standard of care.
Therefore, PSP measurement could be proposed to be included in adults and paediatrics international guidelines to rule out sepsis, in addition to the clinical scores, and in the next definition of sepsis. PSP combined with CRP in adults and PCT in paediatrics could fulfill most of the checklist criteria for an ideal sepsis biomarker presented in the article Sepsis Diagnosis: Clinical signs, Scores, and Biomarkersin this issue of ICU Management & Practice (Table 1).

Disclaimer
Point-of-View articles are the sole opinion of the author(s) and they are part of the ICU Management & Practice Corporate Engagement or Educational Community Programme.
References:
Benninga R, Haquette G, Cateau C et al. (2022) Nanofluidic Technology Enables Rapid Quantification of Pancreatic Stone Protein as an Early Biomarker of Sepsis Method Comparison of the abioSCOPE® In-Vitro Diagnostic Device. 28th AACC International CPOCT Symposium: Meeting Evolving Patient Needs Using Point-of-Care Testing, Montreal.
Cui C, Fu M, Gao B (2017) Procalcitonin and Pancreatic Stone Protein Function as Biomarkers in Early Diagnosis of Pediatric Acute Osteomyelitis. Med Sci Monit. 23:5211-5217.
Eggimann P, Que YA, Rebeaud F (2019) Measurement of pancreatic stone protein in the identification and management of sepsis. Biomark Med. 13(2):135-145.
Evans L, Rhodes A, Alhazzani W et al. (2021) Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Critical Care Medicine. 49(11):e1063-e1143.
Fidalgo P, Nora D, Coelho L, Povoa P (2022) Pancreatic Stone Protein: Review of a New Biomarker in Sepsis. J Clin Med. 11(4):1085.
Graf R (2020) Pancreatic stone protein - sepsis and the riddles of the exocrine pancreas. Pancreatology. 20(3):301-304.
Huo JM, Huo R, Hu L et al. (2017) Value of Procalcitonin, High Sensitivity C-reactive Protein and Pancreatic Stone Protein in Predicting Prognosis of Children with Sepsis. Sichuan Da Xue Xue Bao Yi Xue Ban. 48(3):422-426.
Jiří Ž, Kýr M, Vavřina M, Fedora M (2014) Pancreatic stone protein - a possible biomarker of multiorgan failure and mortality in children sepsis. Cytokine. 66(2):106-11.
Keel M, Härter L, Reding T et al. (2009) Pancreatic stone protein is highly increased during posttraumatic sepsis and activates neutrophil granulocytes. Crit Care Med. 37(5):1642-8.
Klein HJ, Buehler PK, Niggemann P et al. (2020a) Expression of Pancreatic Stone Protein is Unaffected by Trauma and Subsequent Surgery in Burn Patients. World J Surg. 44(9):3000-3009.
Klein HJ, Niggemann P, Buehler PK et al. (2021) Pancreatic Stone Protein Predicts Sepsis in Severely Burned Patients Irrespective of Trauma Severity: A Monocentric Observational Study. Ann Surg. 274(6):e1179-e1186.
Klein HJ, Rittirsch D, Buehler PK et al. (2021b) Response of routine inflammatory biomarkers and novel Pancreatic Stone Protein to inhalation injury and its interference with sepsis detection in severely burned patients. Burns. 47(2):338-348.
Klein HJ, Csordas A, Falk V et al. (2015) Pancreatic stone protein predicts postoperative infection in cardiac surgery patients irrespective of cardiopulmonary bypass or surgical technique. PLoS One. 10(3):e0120276.
Loots FJ, Smits M, Jenniskens K et al. (2022) Added Diagnostic Value of Biomarkers in Patients with Suspected Sepsis: A Prospective Cohort Study in Out-Of-Hours Primary Care. J Appl Lab Med. 7(5):1088-1097.
Niggemann P, Rittirsch D, Buehler PK et al. (2021) Incidence and Time Point of Sepsis Detection as Related to Different Sepsis Definitions in Severely Burned Patients and Their Accompanying Time Course of Pro-Inflammatory Biomarkers. J Pers Med. 11(8):701.
Peng HY, Zhu YM, Zhang XP, Kang XY (2015) Value of pancreatic stone protein/regenerating protein in severity evaluation and prognosis prediction for children with sepsis. Zhongguo Dang Dai Er Ke Za Zhi. 17(11):1183-8.
Prazak J, Irincheeva I, Llewelyn MJ et al. (2021) Accuracy of pancreatic stone protein for the diagnosis of infection in hospitalized adults: a systematic review and individual patient level meta-analysis. Crit Care. 25(1):182.
Pugin J, Daix T, Pagani JL et al. (2021) Serial measurement of pancreatic stone protein for the early detection of sepsis in intensive care unit patients: a prospective multicentric study. Crit Care. 25(1):151.
Que YA, Delodder F, Guessous I et al. (2012) Pancreatic stone protein as an early biomarker predicting mortality in a prospective cohort of patients with sepsis requiring ICU management. Crit Care. 16(4):R114.
Que YA, Guessous I, Dupuis-Lozeron E et al. (2015) Prognostication of Mortality in Critically Ill Patients With Severe Infections. Chest. 148(3):674-682.
Rass AA, Talat MA, Arafa MA et al. (2016) The Role of Pancreatic Stone Protein in Diagnosis of Early Onset Neonatal Sepsis. Biomed Res Int. 1035856.
Rodríguez Rojas C, García de Guadiana-Romualdo L, Morán Sánchez S et al. (2022) Role of Pancreatic Stone Protein as an Early Biomarker for Risk Stratification of Acute Pancreatitis. Dig Dis Sci. 67(7):3275-3283.
Saleh NY, Aboelghar HM, Garib MI et al. (2023) Pediatric sepsis diagnostic and prognostic biomarkers: pancreatic stone protein, copeptin, and apolipoprotein A-V. Pediatr Res.
Satomura Y, Sawabu N, Mouri I et al. (1995) Measurement of serum PSP/reg-protein concentration in various diseases with a newly developed enzyme-linked immunosorbent assay. J Gastroenterol. 30(5):643-50.
Schlapbach LJ, Giannoni E, Wellmann S et al. (2015) Normal values for pancreatic stone protein in different age groups. BMC Anesthesiol. 15:168.
Schlapbach LJ, Graf R, Woerner A et al. (2013) Pancreatic stone protein as a novel marker for neonatal sepsis. Intensive Care Med. 39(4):754-63.
Schneider J, Dick K, Cooper J, Chami N (2022) Pancreatic stone protein point-of-care testing can reduce healthcare expenditure in sepsis. Health Economics Review. 12.
Van Singer M, Brahier T, Brochu Vez MJ et al. (2021) Pancreatic stone protein for early mortality prediction in COVID-19 patients. Crit Care. 25(1):267.
Ventura F (2021) Pancreatic Stone Protein PSP in bacterial superinfection in Covid-19. 39th Vicenza Course on AKI & CRRT Vicenza.
Wu R, Zha L, Hu JH et al. (2017) The value of pancreatic stone protein in the prediction of infected neonates. Minerva Pediatr. 69(6):489-494.
Wu Q, Nie J, Wu FX et al. (2017) Prognostic Value of High-Sensitivity C-Reactive Protein, Procalcitonin and Pancreatic Stone Protein in Pediatric Sepsis. Med Sci Monit. 23:1533-1539.




