
![Tuberculosis Diagnostics: The Promise of [18F]FDT PET Imaging](https://res.cloudinary.com/healthmanagement-org/image/upload/c_thumb,f_auto,fl_lossy,h_184,q_90,w_500/v1721132076/cw/00127782_cw_image_wi_88cc5f34b1423cec414436d2748b40ce.webp "Tuberculosis Diagnostics: The Promise of [18F]FDT PET Imaging")



Executive summary
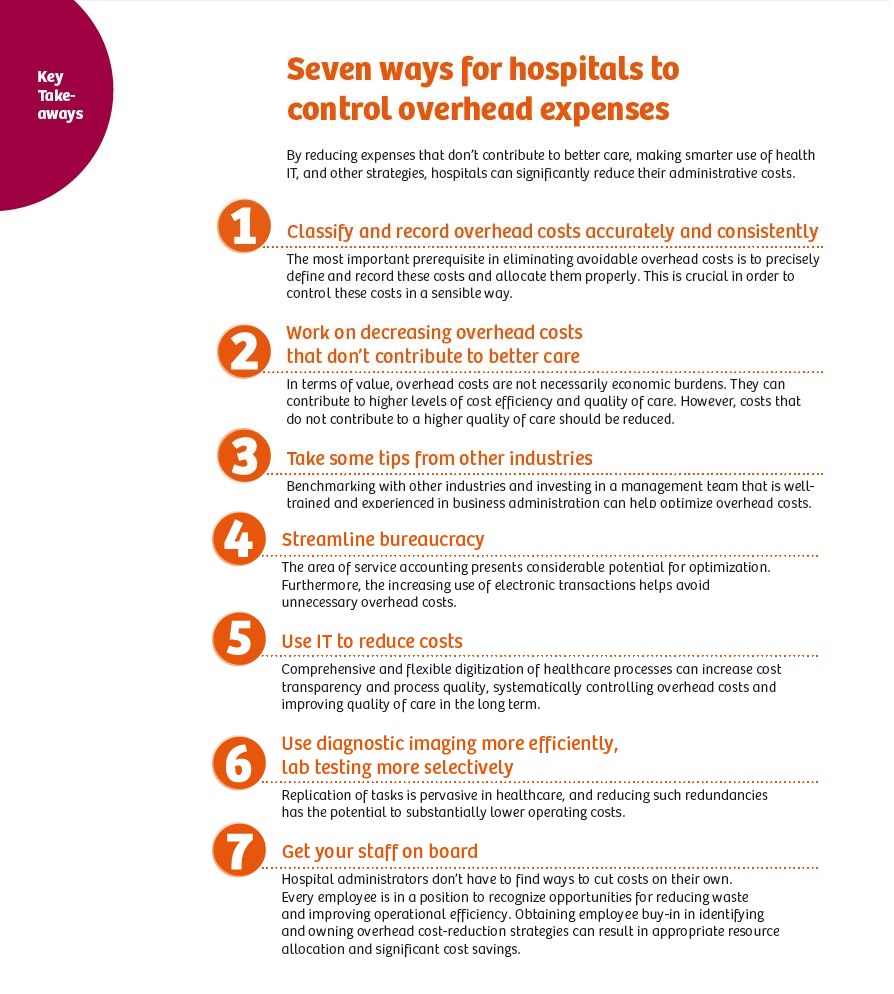
As the costs of caring for patients continue to rise, hospitals all around the world are struggling to contain their operating expenses. This white paper presents seven strategies that successful hospitals have implemented to do just that:
• Tracking and classifying operating expenses
• Reducing operating expenses that don’t contribute to better care
• Applying efficiency practices from other industries
• Streamlining bureaucracy
• Making better use of IT
• Diminishing redundancies in diagnostic testing
• Engaging all staff members in the effort
Introduction
With an ever-increasing volume of sick patients and the constant pressure to contain healthcare costs, hospital administrators are acutely aware of the need to reduce expenses, now more than ever.
Overhead expenses account for a significant portion of total operating costs, which are rising rapidly and represent a ripe target for cost reduction. Hospitals that successfully contain their operating expenses have an immediate advantage over those that do not.
Tackling a problem of this complexity can be stressful, but it must and can be done. As the saying goes, “The greater the obstacle, the greater the glory in overcoming it.” When it comes to healthcare, tackling these challenges head on can often result in even greater rewards. So, are you ready for glory?
In the face of increasing cost pressures and competition, hospitals’ overhead expenses are rising at an unsustainable rate.
Reducing the total cost of care delivery is of vital concern to healthcare providers worldwide. In fact, surveyed U.S. hospitals cited it as the number one area for improvement required to reach financial targets within a three-year time frame.1
Healthcare costs are climbing worldwide at an alarming rate – especially in the United States, where health costs have regularly risen by up to three times the annual rate of inflation since the mid-1960s.2 If the cost of food had undergone a comparable increase, a dozen oranges would cost more than $130 today.3 However, a significant portion of these costs are avoidable. For example, the United States spends $750 billion each year on expenses that are not directly linked to healthcare.4 And according to a study by the consulting firm A.T. Kearney, German hospital doctors spend an average 37 percent of their time on administrative tasks. Among German nursing staff, the average rate is 32 percent, and among medical-technical staff, it is 27 percent.5
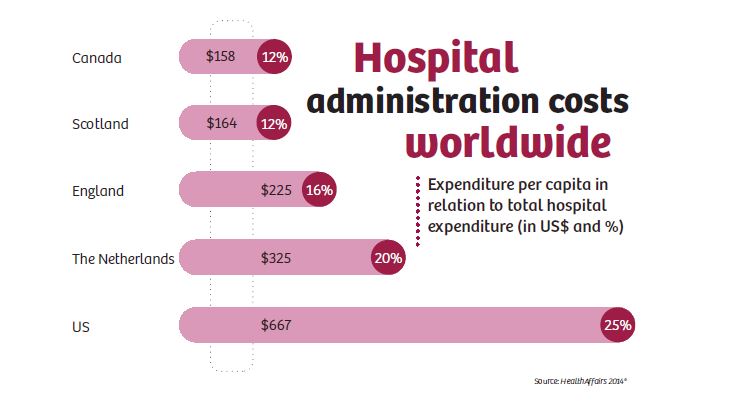
The share of administrative costs differs greatly from country to country. Among other things, this has to do with the varying complexity of health systems and the intensity of competition in each country. A study of hospital administrative costs in several nations finds that hospital bureaucracy consumed 25.3 percent of hospital budgets in the United States in 2011, far more than in other nations, and without any evidence that the high costs translated into better care or yielded any other benefits. Next highest were the Netherlands (19.8 percent) and England (15.5 percent). Scotland and Canada, whose single-payer systems pay hospitals’ operating budgets, with separate grants for capital, had the lowest administrative costs (about 12 percent). According to the study, hospital administrative spending totaled $667 per capita in the United States, $158 in Canada, $164 in Scotland, $211 in Wales, $225 in England, and $325 in the Netherlands. Reducing U.S. per capita spending on hospital administration to Scottish or Canadian levels would have saved more than $150 billion in 2011.6
Healthcare institutions, like other businesses, have certain operating expenses required for the continued function of the business, such as governance and documentation, billing, supplies, energy, rent/property maintenance, transportation, capital charges, cleaning, waste disposal, and other non-clinical personnel expenses. These overhead charges account for a significant portion of total healthcare costs and are, to a certain degree, unavoidable. However, hospital operators who reduce avoidable overhead costs, but also invest in high-value overhead expenses, will increase their institutions’ competitiveness. Here, we examine seven ways in which hospitals may operate more efficiently and get their overhead costs under control.
1. Classify and record overhead costs accurately and consistently
Overhead costs must be captured and classified correctly in order to accurately estimate the costs of clinical versus non-clinical care. “It is critical that the most appropriate allocation statistic is used to allocate overhead costs to the relevant final cost centers or end-product classes,” recommends the Australian-based Independent Hospital Pricing Authority. According to the organization, all costs accumulated in overhead cost centers should be allocated to the final cost to ensure that each product category (patient and non-patient) has its fair share of overhead. This should be done before segregating costs into product categories and, subsequently, into end classes within product categories.7
If overhead costs are not accurately recorded and categorized, this impedes or prevents intervention measures designed to reduce costs. Furthermore, it becomes more complicated to make targeted and useful investments in overhead expenses that could create demonstrable added value.
2. Work on decreasing overhead costs that don’t contribute to better care
In terms of value, overhead costs should not be viewed exclusively as economic burdens. They can contribute to higher levels of cost efficiency and quality of care. However, costs that do not contribute to a higher quality of care, such as certain administrative expenditures, should and must be reduced.
“Managers must make a series of no-regret moves, including maximizing the use of centralizing, outsourcing, and automation. Multihospital networks can achieve efficiency, increase scale, and lower labor costs by centralizing nonclinical, non-differentiating functions such as human resources, marketing, finance, and purchasing,” emphasizes Hospitals & Health Networks Daily. “Individual facilities need to look at employing external expertise and lower cost structures by exploring outsourcing in such areas as information technology, finance, HR, [and] food services.”8
The American Hospital Association (AHA) agrees. In its January 2016 issue of TrendWatch, the AHA advises hospitals to “consolidate administrative processes to achieve economies of scale. Administrative processes are not as unique as individual patients; there are economies of scale in centralizing functions, as many hospitals are learning from consolidation, and/or the adoption of standards to improve administrative and clinical operations across each of their organizational sites.”9
Reining in administrative costs should include consolidating management layers. “If I have four different managers doing the same function, I’m going to get it done four ways,” said Bruce Hallowell, Managing Director at Navigant Healthcare. “This factor alone can run up costs.”10
Shipping costs are another operational area where hospitals can achieve significant cost savings, says Mark Bogen, Chief Financial Officer of South Nassau Communities Hospital in Oceanside, New York. A few years ago, he noted that his hospital’s inbound shipping costs averaged around $500,000 per year. Subsequently, South Nassau was able to save $75,000 by simply leveraging its buying power with carriers. Hospitals can also save thousands of dollars by reducing overnight shipping for operating room supplies.11 In addition, hospitals can achieve significant overhead expense reductions by investing in more efficient facilities. Kay Winokur, Resident Nurse and Vice President of Quality, Safety, and Accreditation at Beaumont Health System in Royal Oak, Michigan, says that her institution has reduced costs significantly by improving landscaping irrigation (saving $180,000 during each six-month watering season), investing in energy-efficient lighting and fixtures (saving $900,000 every year), revamping its chilled water distribution systems (saving $37,000 per year), installing solar panels in sunny areas (saving $12,000 over a three-year period), replacing inefficient sinks, toilets, and urinals (saving $257,000 annually), switching to new, more cost-effective recycling initiatives, and using timers to heat coffeepot water only during business hours. Even an item as small and simple as a coffeepot was able to save the Beaumont Hospital System $34,000 per year.11
3. Take some tips from other industries
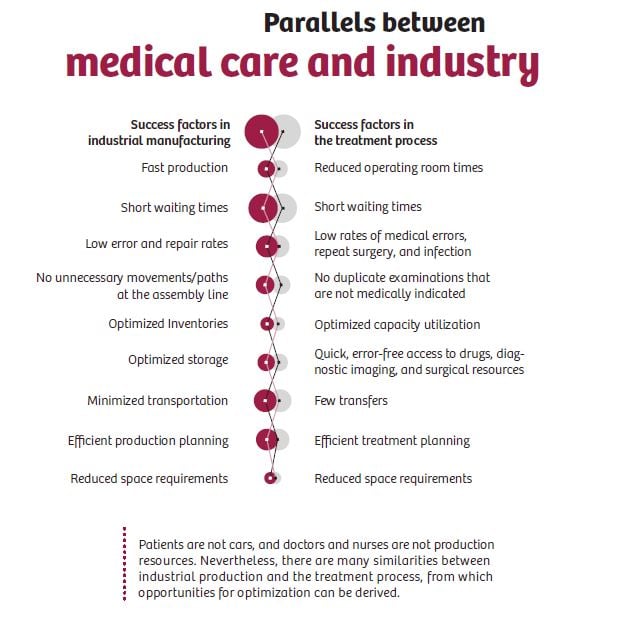
Despite the high degree of flexibility required to run a hospital, there are also many opportunities to learn from other industries – manufacturing, for example – in the area of just-in-time concepts. It would be wise for healthcare providers to look at successful cost-efficiency measures currently being used by other industries.
For example, industrial production defines value with measures such as short throughput, optimal utilization, minimum downtime, short transport routes, low storage costs, low error rates, and a comprehensive knowledge of current stock quantities and the location of production resources. These measures are undisputed determinants of success, with high levels of attention and planning devoted to them. However, the situation in healthcare is often very different. For years, hospitals have accepted declining bed occupancy rates (averaging 77 percent in Germany in 2014 and 67 percent in the United States in 2011) in conjunction with regular overcrowding at peak times. Attempts to schedule elective surgeries at low-utilization times, for example, often appear unsuccessful at resolving this paradigm.
Standardizing U.S. hospitals’ billing operations for physician and clinical services could save $26 billion, according to James L. Heffernan from the Massachusetts General Physicians Organization. Comparing the administrative costs of a single professional billing office to that of Medicare, he concluded that a single transparent set of payment rules in a multi-payer healthcare system would potentially save money, as well as four hours per physician per week and five hours of practice support staff time per week.13
In addition to emulating the lean efficiency approaches that other industries have used to optimize operations, hospitals may also benefit from other cost-control initiatives currently being embraced by employers worldwide, such as encouraging wellness among their own employees. The Community Hospital of the Monterey (California) Peninsula (CHOMP) implemented a new wellness and disease management program for its staff to provide better oversight and education about chronic health problems, such as diabetes and asthma. CHOMP’s employees now receive financial incentives in the form of lower health insurance premiums for completing the wellness program or showing improvement in five main wellness categories. In 2009, CHOMP’s monthly health costs were $705.65 per member; in 2012, that figure dropped almost 15 percent to $602.25 per member per month. “We’re making it easier for employees to [take care of themselves], and it has saved us millions of dollars per year,” says Laura Zehm, Chief Financial Officer of CHOMP.11
4. Streamline bureaucracy
All over the world, hospital operators are working under the burden of excessive complexity and bureaucracy. Even a seemingly straightforward activity such as filling a prescription order is fraught with unexpected intricacies. In the United States, for example, it can be accomplished in 786 different ways, involving a number of different healthcare professionals and technical channels. Managing the requirements of many different health-benefit plans places a heavy administrative burden on clinicians.4
One of the most effective ways to reduce overhead costs is to optimize the recording and billing of services provided. In Germany, for example, one of the main reasons for the heavy administrative workload of medical staff is discharge letters, which include correctly coding diagnoses and procedures and entering this data into the hospital information software.14 This extensive manual process must then be further processed by hospital administration staff.
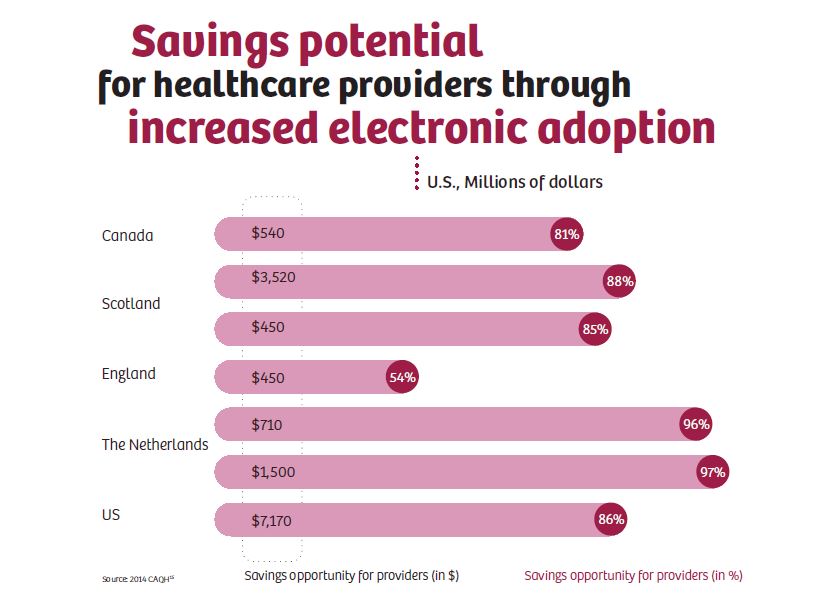
In the United States, healthcare providers handled more than 2.4 billion transactions manually in 2013. On average, only 72 percent of eligible transactions are performed electronically.15 However, average adoption rates of fully electronic transactions varied widely, from 92 percent for claim submission to just 7 percent for prior authorization.
The potential for significant cost savings is enormous due to the large volume of transactions and the dramatic cost difference between manual and electronic transactions. Healthcare providers estimated that costs per transaction averaged more than $5 for a manual transaction and approximately $1.60 for each electronic transaction. The findings indicate that U.S. healthcare providers could save approximately $7 billion annually by transitioning six routine business transactions (i.e., claim submission, eligibility and benefit verification, prior authorization, claim status inquiry, claim payment, and remittance advice) from manual to electronic.16 This represents an average savings potential of 86 percent when compared to the costs of manual transactions.
Billing represents a great source of expense for hospitals, as does attempting to collect on bad debt. Hospitals that educate their patients on the billing process are more likely to have complying patients and avoid protracted disputes and bad debt. Chad Sandefur, Director and Healthcare Analyst for AArete, a global management and consulting company, explains that ensuring patients develop this knowledge is critical – “By training staff to collaborate with patients and to educate them early, it removes the surprises when the bills come, and that facilitates the payment component.”17
In addition, hospitals in the United States lose billions of dollars each year from incorrect invoices to cost bearers. According to the American Medical Association’s National Health Insurer Report Card, one in every five medical claims is processed inaccurately by commercial health insurers. A 20 percent error rate represents a level of inefficiency that wastes an estimated $15.5 billion in claims that are never corrected and reprocessed.18
“Eliminate redundancy in financial process to eliminate redundant manual paper- and phone-based legacy processes with health plans, and replace these with automated routines,” recommends the AHA. Furthermore, the AHA notes that currently, providers often have to pursue multiple time-consuming avenues to confirm patients’ eligibility, deductibles, and copay amounts.18
Another option is to outsource the receipt of payments from automotive insurers and workers’ compensation programs. “To reduce healthcare revenue cycle management (RCM) costs, hospitals should consider outsourcing their workers’ comp and automotive insurance payments management to parties that provide health billing services, manage attorney correspondence, negotiate claims, and conduct other administrative responsibilities,” says ProMedical. “According to Black Book Market Research, 54 percent of healthcare financial executives believe outsourcing RCM enables them to increase efficiency and improve fiduciary well-being.”16
5. Use IT to reduce costs
Healthcare is challenged by large amounts of data that is diverse, unstructured, and growing exponentially. Data constantly streams in real time, through interconnected sensors, monitors, and instruments. By 2016, 4.9 million patients worldwide were projected to use remote monitoring devices.19 Even in 2010, an average U.S. hospital already had to manage one billion terabytes of data. The amount of data is expected to rise by a factor of 50 from 2014 to 2020. Combined with a growing need for providers and payers to retrieve, analyze, and share data, it’s clear why healthcare organizations must consider migrating from their traditionally fragmented technology
infrastructure to cloud-based solutions.20
However, today’s IT systems and their concepts are often too rigid, operate as standalone solutions, and are not interconnected. “The structure of the system makes it difficult, if not impossible, to establish binding communication processes solely between protagonists that are directly involved,” writes A.T. Kearney.5 “Competent treatment support that serves the patient must be established across existing boundaries of care. Only carefully coordinated processes within the system can guarantee an accurate management of processes.” The authors added that communication processes through third parties should be eliminated by employing lean information flows that reduce interfaces and save costs.
In many countries, a major hurdle lies in the narrow legal restraints for collecting, storing, and disseminating data, which thwarts technically feasible leaps in development and cost reductions in the administrative sector and elsewhere. For instance, in Germany, an extensive network of databases and access to such facilities would currently be prohibited on privacy grounds.5 National and European initiatives (e.g., eHealth – secure digital communications in healthcare) are addressing this issue by aiming to provide a technically and legally sound foundation.
Comprehensive and flexible digitalization of hospital processes is essential in order to enhance efficiency, counteract the overhead cost induced by complexity, and improve transparency.
“Move fully to electronic processes,” says the AHA. “When providers utilize the transaction standards and operating rules to establish automated routines for the handling and posting of data, they can benefit from better and more timely data, reduced operating costs, and improved patient satisfaction.”18
The AHA adds that hospitals must establish expectations with vendors to ensure that they keep pace with system changes and that systems be upgraded to accommodate standards and operating rules. However, the United States’ Health Information Privacy and Accountability Act (HIPAA) does not require vendors to be in compliance with the transaction standards and operating rules. In order to support HIPAA standards and operating rules in a timely manner, customers must demand that vendors implement changes. “Examine your vendor contracts to ensure they include language requiring timely updates and demonstrated compliance with standards and operating rules,” the AHA advises, adding that vendors can demonstrate support for compliance by voluntarily certifying their products with the Council for Affordable Quality Healthcare’s Committee on Operating Rules for Information Exchange.21
A case study from Asia shows how structural and IT initiatives help reduce overhead expenses and also improve outcomes, as well as the overall financial performance, of a hospital. In 2008, Singapore’s Ministry of Health set up the Agency for Integrated Care to reform long-term care delivery, particularly for the city-state’s soaring elderly population. Among the initiatives was the Singapore Programme for Integrated Care for the Elderly (SPICE), a community program that uses both local care centers and home care to enable frail elderly patients to be cared for in the community instead of in a hospital, and Holistic Care for Medically Advanced Patients, a program that provides palliative care in patients’ homes. Through the use of Electronic Hospital Records (EHRs), eligible patients are accurately assigned to one of the two initiatives. Funding models, including capitated monthly payments, allow providers to pool and redirect resources toward care reforms that improve outcomes while also facilitating patient transitions to appropriate care settings. The funding model supports Aged Care Transition teams to help ensure the coordinated delivery of care after a hospital discharge. The teams consist of transition coordinators who access national EHRs, which are linked to patient registries, track all relevant patients, and transition them from a hospital to an optimal care setting. The transition coordinators manage referrals of patients and supply integrated information for case management to other providers, with a particular focus on high-intensity hospital users.
The outcomes have been positive. The Aged Care Transition teams have reduced 30-day hospital readmission rates by more than 40 percent. SPICE has halved the number of emergency department visits among its population. The annualized savings attributed to the Aged Care Transition program has been 17,000 hospital-days, worth more than $11 million.22
6. Use diagnostic imaging more efficiently, lab testing more selectively
Computed tomography, magnetic resonance tomography, X-rays, and other forms of imaging generate large volumes of data. A significant portion of the information collected in imaging diagnostics remains unused because it is stored in different formats and at different locations, among other things. Experts estimate that using all of this data efficiently could save hundreds of billions of overhead dollars in the United States healthcare industry alone.23
A systematic networking of diagnostic imaging equipment, as well as the overarching analysis of operational data, can give large hospitals, hospital groups, and diagnostic centers an overview of their equipment fleet utilization. Information about the nature, timing, and duration of the examination could be used, for example, to optimize the utilization of the devices. Hospital groups could determine whether each piece of equipment is being used efficiently and for the right examinations at its current location. Workflows could also be improved. For example, body coils have to be rearranged for different magnetic resonance imaging investigations. Knowing the time this takes allows for a more efficient and tighter organization of scanning sequences. Similarly, redundant laboratory testing has been estimated to waste up to $5 billion each year in the United States, according to the American Journal of Clinical Pathology. “Laboratory testing is one factor that contributes to rising healthcare expenditures,” according to the journal’s researchers. “It is becoming increasingly evident that cost stabilization and reduction, including within-laboratory services, are necessary to place our nation’s healthcare system back on a sustainable course.” In order to prevent unnecessary laboratory testing, providers should be cautious when first ordering tests. Computerized physician order entry systems that allow for system-defined rules for utilization management would help physicians order tests more effectively.11
7. Get your staff on board
The Harvard Business Review recommends that hospitals align any cost-cutting initiatives with their organizations’ mission and culture, and then engage clinical and administrative staff across their organizations to collaborate in the process. Banner Health, one of the United States’ largest health systems, experienced substantial declines in patient volume during the financial crises, along with reductions in reimbursements, amounting to hundreds of millions of dollars.
Nonetheless, between 2012 and mid-2013, Banner Health captured nearly $70 million in cost savings with the aid of its entire staff. By 2017, the savings from these efforts is expected to contribute $256 million annually to Banner Health’s bottom line. Banner Health’s 10-member senior leadership team used a variety of channels, such as town halls and videos of executives, to clearly and repeatedly communicate the urgent need for cost reduction and system-wide process redesign strategies to improved patient care. This helped squelch rumors of impending layoffs and reduced the stress and fear that accompany cost-cutting discussions. The leadership team described how cutting costs would enable the system to invest in new initiatives, such as an accountable care organization and a network of community-based outpatient clinics, which enabled Banner Health to better coordinate, standardize, and integrate care delivery, eventually improving population health. Finally, they invited people from across the system to collaborate in cost-reduction strategies. They wanted physicians, administrators, line managers from different facilities, department managers, and staff to work together to find innovative solutions that would cut costs, while simultaneously enhancing patient experience, clinical quality, and financial sustainability.
In alignment with this collaborative approach, eight cross-functional teams were formed. Each team analyzed the cost structure of one particular function and then recommended cost-reduction tactics. The pilot resulted in a day-long meeting with the senior leadership reviewing 123 recommendations, of which 116 – valued at $104 to $133 million annually, or 18 to 24 percent of Banner Health’s general and administrative expenses – were approved. These included opportunities to deploy more self-service technology supported by a shared services organization, saving nearly $4 million in HR administrative costs; insource second physician reviews of inpatient charts, saving nearly $8 million; and create an internal facility for drug compounding and packaging, saving up to $3.5 million. By the end of 2012, the first year of implementation, Banner Health captured $31 million in general and administrative savings. The decision to be inclusive and collaborative was essential to generating these savings and ensuring support from frontline leaders and staff.24
In a similar initiative, Children’s Hospital at the Medical University of South Carolina introduced a new expectation for all of its staff members and leaders: spend 80 percent of working time on completing necessary tasks and the other 20 percent on finding ways to do them more safely and more efficiently. Many successful ideas were generated by frontline staff, managers, and physicians, to reduce waste, standardize practices, and reduce avoidable complications.
These cost-saving efforts included:
• Creating standard order sets and reducing the amount of chemotherapy and supportive care agents wasted
• Reducing overtime, which resulted in an annual savings of $150,000
• Reducing the cost per clinic visit by standardizing scheduling templates, consolidating clinics, and changing staffing models, producing an annual savings of more than $250,000
These efforts produced additional measurable outcomes, including:
• 19% reduction in overtime costs per pay period
• 17% reduction in costs per case
• 30% reduction in pharmaceutical costs per case
• 15% reduction in lab costs per case
• 11% reduction in length of stay
• 6.5% reduction in ventilator days per adjusted discharge 25
References
1. Healthleaders Media. (2014.) Industry Survey 2014: Forging Healthcare’s New Financial Foundation. January 2014. http://www.healthleadersmedia.com/report/intel/2014-industry-survey-forging-healthcares-new-financial-foundation. Accessed January 27, 2017.
2. Deutsches Ärzteblatt. (2001.) Managed Care in den USA: Übermacht der Versicherungen. http://www.aerzteblatt.de/archiv/29918. Accessed January 27, 2017.
3. Institute of Medicine. (2011.) The Healthcare Imperative: Lowering Costs and Improving Outcomes – Workshop Series Summary. February 24, 2011. http://www.nationalacademies.org/hmd/Reports/2011/The-Healthcare-Imperative-Lowering-
Costs-and-Improving-Outcomes.aspx. Accessed January 27, 2017.
4. Institute of Medicine. (2012.) Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. September 6, 2012. http://www.nationalacademies.org/hmd/Reports/2012/Best-Care-at-Lower-Cost-The-Path-to-Continuously-Learning-Health-Care-in-America.aspx. Accessed January 27, 2017.
5. Scheel O., Thiry E., Schmidt-Rhode C., Berenbeck M. (2011.) Deutsches Gesundheitssystem auf dem Prüfstand: Kostenfalle Komplexität. A.T. Kearney. Düsseldorf, Germany. December 2011.
6. Himmelstein DU, et al. (2014.) A Comparison of Hospital Administrative Costs in Eight Nations: US Costs Exceed All Others by Far. HealthAffairs. September 2014.
7. The Independent Hospital Pricing Authority (IHPA). (2014.) Hospital Patient Costing Standards. July 2014. https://www.ihpa.gov.au/sites/g/files/net636/f/publications/ahpcs-version3.1.pdf. Accessed January 27, 2017.
8. Kaul A. (2014.) A Belt-Tightening Regimen for Hospital Systems. Hospitals & Health Networks Daily. August 7, 2014. http://www.hhnmag.com/articles/4067-a-belttightening-regimen-for-hospital-systems. Accessed January 27, 2017.
9. American Hospital Association TrendWatch. Administrative Simplification Strategies Offer Opportunities to Improve Patient Experience and Reduce Costs. January 2016. http://www.aha.org/research/reports/tw/16jan-tw-adminsimp.pdf. Accessed January 27, 2017.
10. RevCycle Intelligence. (2016.) Ways to Cut Costs through Hospital Revenue Cycle Management. May 16, 2016. http://revcycleintelligence.com/news/5-ways-to-cutcosts-through-hospital-revenue-cycle-management. Accessed January 27, 2017.
11. Herman B. (2013.) 9 Ingenious Ways to Cut Costs at Your Hospital. Becker’s Hospital Review. February 26, 2013. http://www.beckershospitalreview.com/finance/9-ingenious-ways-to-cut-costs-at-your-hospital.html. Accessed January 27, 2017.
12. Fischlein J., Pfänder T. (2007.) Industrielles Klinikmanagement: Moderne Management-Prinzipien übertragen auf aktuelle Herausforderungen in Kliniken. October 31, 2007. FinanzBuch Verlag, München.
13. Reisenwitz C. (2015.) The Secret to Reducing Hospital Administration Costs. EMR. July 23rd, 2015. http://blog.capterra.com/the-secret-to-reducing-hospitaladministration-costs/. Accessed January 27, 2017.
14. Scheel O., Thiry E., Schmidt-Rhode C., Berenbeck M. (2011.) Deutsches Gesundheitssystem auf dem Prüfstand: Kostenfalle Komplexität. A.T. Kearney. Düsseldorf, Germany. December 2011.
15. 2014 CAQH Index™: Electronic Administrative Transaction Adoption and Savings, Calendar Year 2013. http://www.caqh.org/sites/default/files/explorations/index/report/2014Index.pdf. Accessed January 26, 2017.
16. ProMedical. (2016.) 3 Ways to Reduce Hospital Revenue Cycle Management Costs. December 20, 2016. http://promedllc.com/billing-resolutions/3-ways-to-reducehospital-revenue-cycle-management-costs/. Accessed January 27, 2017.
17. Healthcare Information and Management Systems Society (HIMSS). (2015.) Navigating the Healthcare Reimbursement Process. August 17, 2015. http://www.himss.org/news/navigating-healthcare-reimbursement-process. Accessed January 26, 2017.
18. American Hospital Association TrendWatch. (2016.) Administrative Simplification Strategies Offer Opportunities to Improve Patient Experience and Reduce Costs. January 2016. http://www.aha.org/research/reports/tw/16jan-tw-adminsimp.pdf. Accessed January 26, 2017.
19. IBM, Berg Research. (2015.) Big Data in Healthcare: Tapping New Insight to Save Lives. http://preview.thenewsmarket.com/Previews/IBM/DocumentAssets/279328.pdf. Accessed January 26, 2017.
20. Accenture. (2015.) Healthcare IT: Top Five Digital Trends Fueling Disruption in Healthcare.
21. American Hospital Association TrendWatch. (2016.) Administrative Simplification Strategies Offer Opportunities to Improve Patient Experience and Reduce Costs. January 2016. http://www.aha.org/research/reports/tw/16jan-tw-adminsimp.pdf. Accessed January 27, 2017.
22. McClellan M., et al. (2015.) Accountable Care Around the World: A Framework to Guide Reform Strategies. Health Affairs. September 11, 2015.
23. McKinsey Global Institute. (2008.) Accounting for the Cost of U.S. Health Care: A New Look at Why Americans Spend More. December 2008. http://healthcare.mckinsey.com/sites/default/files/MGI_Accounting_for_cost_of_US_health_care_full_report.pdf. Accessed January 27, 2017.
24. Dahlen D. & Bailey C. (2013.) Cutting Costs Without Cutting Corners: Lessons from Banner Health. Harvard Business Review. October 18, 2013. https://hbr.org/2013/10/cutting-costs-without-cutting-corners-lessons-from-banner-health. Accessed January 27, 2017.
25. Rees C. (2014.) How Hospitals Can Save 18 Percent in Direct Costs. Children’s Hospitals Today. July 13, 2014. https://www.childrenshospitals.org/newsroom/childrens-hospitals-today/issue-archive/issues/summer-2014/articles/how-to-save-18-percent-in-direct-costs. Accessed January 27, 2017.




