HealthManagement, Volume 21 - Issue 5, 2021
 PRINT OPTIMISED
PRINT OPTIMISED
The “Digital Anamnesis” concept and the proposed model may have useful implications for medical education, in a medical practice and for conceptualisation of modern Electronic Health Records
Key Points
- Medical history taking is a historically, and key part of clinical practice and provides a correct diagnosis 76% of the time, when performed correctly by a doctor.
- History taking is reliant on information provided by the patient and/or the next of kin. Aging populations may suffer from memory loss, which may cause issues with information recall.
- As anamnesis means a patient’s account of a medical history, the process of medical history taking using digital means would be designated Digital Anamnesis.
- Data management is fundamental in a physician’s practice of digital anamnesis. A systematic and oriented data extraction is directly related with increased productivity and efficiency.
- Physicians’ training is a necessary step when implementing and using digital health tools and systems such as EHR. When utilised properly, it may be possible to reduce “click fatigue” and physicians’ workload.
Introduction
Medical history taking has been a pillar of clinical practice for many centuries. Even now it is estimated to provide a correct diagnosis 76% of the time, when performed by a doctor with adequate communication skills (Seitz T et al. 2019). But history taking has remained mostly reliant on information provided by the patient and/or the next of kin. With the increase in life-expectancy, populations have more complex and chronic diseases which are often are associated with conditions such as dementia or age-associated progressive memory loss, which may significantly hamper the capacity for information recall and reporting (Prince et al. 2013; European Commission 2021).
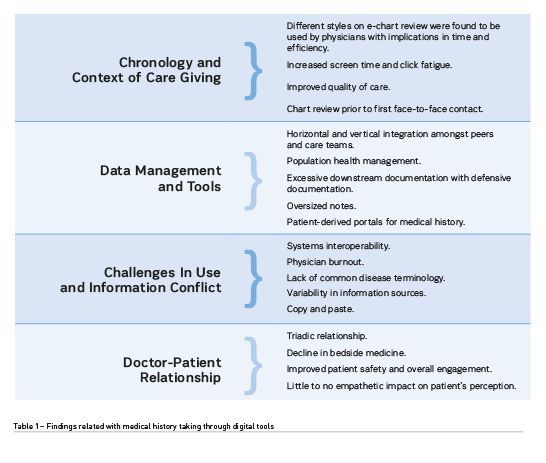
Digital tools in clinical practice mean new tools for physicians to provide care. One such is the possibility to gather and store information related with care giving in online, interoperable systems. This, however, has brought changes in workflow and occasionally with risk for increased workload and fatigue (Martins 2007). Table 1 summarises findings in current literature reviews regarding use of digital tools in medical history taking (Lino and Martins 2021; Hedian et al. 2018).
Digital Anamnesis
As highly variable workflow adaptations have been found, we propose that the existence of a common referential could promote more harmonised medical history taking when exploring digitally stored information. As anamnesis means a patient’s account of a medical history, the process of medical history taking using digital means would be designated Digital Anamnesis. Having a clear concept and a basic model for this is very important as this can of course be further matured, but serves to guide current clinical practice and education. Establishing a framework to help harmonise digital tool use, caregiving and workflows, may improve patient safety, physician’s satisfaction, and workload and productivity management. A preliminary model for Digital Anamnesis has been developed based on current classic medical history taking models (Evans et al. 1993; Kurtz et al. 2003). It stems from the interconnection of three major components:
The first is the content of the medical history to be explored via digital tools. As classic medical history relies on the patient’s ability to recall information related with the chief complaint, history of the present complaint, past medical history, family, personal and social history, drug and allergy history, functional enquiry/systems review. Digital tools have the possibility to build a virtual construct of the patient based on this information – a sort of “iPatient”. This allows for the data stored within the EHRs to be systematised and facilitate the interpretation of the background in which the patient is inserted.
The second component is the skills set needed for the exploration of data. As physicians are the main sources of data input and output, they are required to be competent in information gathering and introduction. Thus, computer skills and literacy, multitasking and documentation managing and data selection skills for note review and entry heavily impact physicians’ relationship with digital tools.
Physicians’ training is a necessary step when implementing and using digital health tools and systems such as EHR. Not only is it beneficial to include written and reference material to guide the provider, but also practical lessons and opportunities should be available. This should not happen only once, but rather continuous training may improve efficiency and productivity when updates or changes are introduced in the system.
Data management is fundamental in physician’s practice of digital anamnesis. A systematic and oriented data extraction is directly related with increased productivity and efficiency. Physicians need to be educated in data input and output. Utilising the right templates to introduce the adequate information leads to easier data extraction. When conducting chart reviews, it may be possible to reduce time consumption, also known as “click fatigue” and physicians’ workload.
Basic computer skills are acquirable traits that influence physician’s relationship with digital tools. As defined by UNESCO “Basic computer skills courses cover the most common usages of a computer, including a majority or all of the following: understanding the basic notions of computer manipulation; managing computer files, word processing, using spreadsheets and databases; creating presentations; finding information and communicating using computers; and being aware of social and ethical implications of Internet use.” (UNESCO UIS 2021). When considering EHR usage, the provider must be able to interact with the system without the need for advance computer manipulation skills.
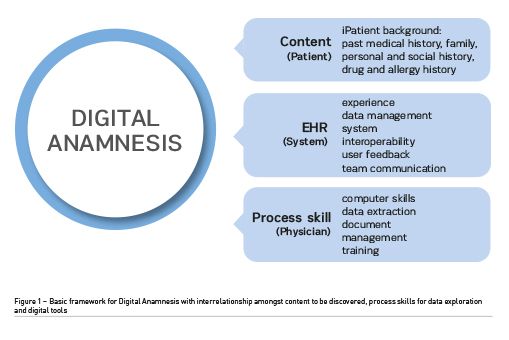
Lastly, the interface and tools used also impact the possibility and methods for digital medical history taking. User interface, system interoperability and data management are factors that influence efficiency when considering physicians’ and digital tools relationship.
Discussion
User experience and interface influence physician’s ability to quickly access information. Through user-friendly tools such as shortcut and search bars, information preview, and technical support, productivity can be increased, and fatigue decreased. It also allows data to be more readily accessible when conducting chart review. Physician’s feedback should be a valuable tool when designing and reassessing EHR, contributing to system development directly.
Adequate template design can allow for intuitive data input and extraction. Medical specialty and setting of care should influence software design and architecture. As different necessities arise from urgent to inpatient to outpatient care.
Team communication and system interoperability increase information available and improve digital medical history accuracy. It also provides information from different types or care from nutritionist, to nursing, to medical information. Providers can then gather data to induce a holistic approach to care giving. Increasing patient safety and satisfaction and quality of care.Patient-derived information in EHR can also be found in some systems. This allows far greater data collection and accuracy. Nonetheless, perhaps even more fundamental than conceptualising a purely digital process of medical history taking is the consideration that doctors will need to be proficient in conducting Digital Anamnesis and hybridising it with Classic Anamnesis. As both sources can complement each other allowing for a meticulous medical history.
Conclusions
Future work is needed to evaluate possible models and templates of Digital and Classical Anamnesis hybridisation. Those can be implemented in clinical practice and medical education, such as the room used for simulations labs at UBI Medical School (Sa 2011). Medical educators should integrate this concept in students’ curriculum. Future physicians’ will most likely continue to rely on different digital tools to develop their practice. Furthermore, multiple associations such as the Association of American Medical Colleges (Obeso et al. 2017) have advocated that digital tool skills are necessary for junior interns. Digital tools developers may integrate this information during system development stages where priority to user friendliness and data management and security can be a point of focus.
Conflict of Interest
None. 
References:
European Commission (2021) The 2021 Ageing Report. Economic & Budgetary Projections for the EU Member States (2019-2070). Vol. 148. 2021. 375 p.
Evans BJ, Sweet B, Coman GJ (1993) Behavioural assessment of the effectiveness of a communication programme for medical students. Med Educ. 1993;27(4):344–50.
Hedian HF, Greene JA, Niessen TM (2018) The Electronic Health Record and the Clinical Examination. Med Clin North Am. 2018;102(3):475–83.
Kurtz S, Silverman J, Benson J, Draper J (2003) Marrying content and process in clinical method teaching: Enhancing the Calgary-Cambridge guides. Acad Med. 2003;78(8):802–9.
Lino L, Martins H. (2021) Medical History Taking Using Electronic Medical Records: A Systematic Review. 2021;(X):1–11.
Martins HMG (2007) Caregiver-patient-information system triad: Conceptualising the workspace for mobile and ubiquitous computing in Health. Heal 2007 Ubiquitous Heal Aging Soc - 2007 9th Int Conf e-Health Networking, Appl Serv. 2007;299.
Obeso V, Brown D, Phillipi C, Aiyer M, Barron B, Bull J, et al. (2017) Core entrustable professional activities for entering residency Pilot Program. Toolkits for the 13 Core Entrustable Professional Activities for Entering Residency. 2017;20.
Available from: aamc.org/download/484778/data/epa13toolkit.pdf
Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP (2013) The global prevalence of dementia: A systematic review and metaanalysis. Alzheimer’s Dement [Internet]. 2013;9(1):63-75.e2. Available from: dx.doi.org/10.1016/j.jalz.2012.11.007
Sa J (2011) Teaching Non-technical Skills through Medical Simulation – Master Thesis, full text available at: ubibliorum.ubi.pt/bitstream/10400.6/1051/1/Tese%20Final.pdf
Seitz T, Raschauer B, Längle AS, Löffler-Stastka H (2019) Competency in medical history taking—the training physicians’ view. Wien Klin Wochenschr. 2019;131(1–2):17–22.
UNESCO UIS [Internet] (2021) Basic computer skills [cited 2021 Jun 17]. Available from: uis.unesco.org/en/glossary-term/basic-computer-skills

