HealthManagement, Volume 18 - Issue 6, 2018
 PRINT OPTIMISED
PRINT OPTIMISED
Patient-driven data business, not data-driven patient business.
Data-driven business models make up the medical and healthcare market in large parts, a trend reinforced by further technological developments and regulation. Care must be taken to avoid a situation where only a few players benefit.
Who lives outside the GAMFANNAT economy (Google, Apple, Microsoft, Facebook, Amazon, Netflix, Alibaba, Tencent)? An increasing market capitalisation of approximately $5 trillion (July 2018)—a multiple of the market value of all German Stock Exchange 30 companies together—and an even deeper connection of services and products with our increasingly digitally organised and experienced life clearly show that large parts of the global consumer society today and even more tomorrow and the day after tomorrow will become data-driven spheres. It is easy to imagine a world without fossil fuel-powered automobiles, but with flying autonomous vehicles—a bit harder without cell phones, and with brain implants. A world without data in the sense of their intensive generation and usage, in all areas of life seems to be hardly tangible (unless as a conscious and fairly complete renunciation of technology).
You might also like: Smart hospital ethics: starting the dialogue
The development of data-driven activities as a whole is increasingly ethically questioned. In Germany, the Data Ethics Commission has recently been created within the Federal Ministry of Interior, Building and Community, and in England the Data Ethics Framework of the Department for Digital, Culture, Media and Sport. Today, it is unimaginable not to use digital advances in medicine, which are certainly critical in ethical terms, yet impressive, especially data-driven ones, for positive precaution, diagnosis, healing and aftercare opportunities for patients and healthy people. From AI in radiology to precision medicine in oncology, people want to be, become, and stay healthy. Here a peculiar tension erupts.
In the GAMFANNAT world, considerably more people are using the services offered than would be expected in view of the level of trust that users have in their data usage—apart from the fact that hardly anyone, for example, really works through, understands or can decipher privacy statements. Transparency as a condition of the opportunity for fair consent looks different. To put it clearly: The GAMFANNAT Grandpa should not be sitting next to Lehman Granny. Nor is it to be expected that, in the end, patients will not give priority to the medical benefit of their data because of concerns about a "patient credit bureau", even if the treatment contexts are hardly accessible to the individual patient. Convenience has always limited data protection requirements in real terms, and data protection should not be a luxury for the healthy. In addition, the GAMFANNAT players are already today—recognisable openly or only in contours—increasingly active in the medical and healthcare market and game changers.
What data-related opportunities and risks arise for patients from a business perspective? How can patients not only be masters of their data, but use data business cases for themselves? What is the value of their medical and health-related data? Which commercial, social or individual medical use of personal data makes sense and is as safe as it can be in the digital realm?
Economically, data is neither oil nor currency – but nevertheless the central future exchange unit for patients
Economically, oil is private property with exclusive ownership. My oil is my oil. Only I can use it, nobody else. When it's used up, it's gone, and I can only use one litre of oil to the extent of one litre of oil. If I mix 1,000 litres of oil, it won’t become "super oil". In economic terms, data have a completely different nature. I can share my data with multiple users, so they are not rivals, and when many different pieces of data come together, they create network effects that can in part lead to significant benefit increases. In addition, data can be copied virtually unlimitedly, does not wear out, can be transferred, and can be handled through access, use, and change, and distinguished into private club goods or public data assets (eg weather data). And you can do amazing mathematics with it: statistics is the new basic subject for understanding the data economy.
My personalised medical data may only have limited economic value for me—which may be existential—but economically cannot be increased arbitrarily. However, for a company, various data such as my personalised but also impersonalised data (anonymised, pseudonymised, or purely machine-generated) can, when aggregated, lead to completely new insights and offers, and in the end even to innovative value added. In modern data medicine, such effects are currently on the agenda, and therefore, for example, for the pharmaceutical industry, of great interest.
The emancipation of correlation versus causality does not take place in strict scientific theory, but in the pragmatic world of business models—even with seriously anonymised data, cross-referencing and correspondingly smart data analysis models can often compensate for the information about the person that has been legally deleted, provided that those data are cleverly combined with other data (eg data from search engines or fitness devices). It is known that 87 percent of the US population can be re-identified by the combination of zip code, gender and date of birth (Sweeney 2002). Precisely because my data does not generally represent a significant value for me, there was—and is—a tendency to pass it quite relaxed to the companies in exchange for services and products. That's just how it is as a consumer: “If you are not paying for it, you're not the customer; you're the product being sold” (Lewis 2012).
To a large extent the enormous market value of the corresponding data-driven companies is explained. Because they do not really share the cake. With a view to patients, this trend slowly begins to gain contours in the medical and healthcare sector. Strictly speaking, the medical data of patients is not a currency for patients themselves, because they are not a constant reference value, but depend essentially on their context. However, data can replace financial transactions via their specific value—and yet, no oil, no currency, but an economic value that should be repaid.
Business models for the use of medical data and ideas for determining the value of data are diverse and rarely recognisable today
Which business models in the medical and healthcare industry use data and how is this money earned? This very simple-sounding question says it all. In principle, data can be traded or used directly (or as in the case of open data provided without consideration, or data sharing). The GAMFANNAT economy usually does the latter and thus comes to steadily richer and deeper user experiences and increased, individual benefit, leading to a corresponding willingness to pay and, above all, loyalty—and last but not least, to competitive advantages. The algorithms of the companies are ultimately unregulated and in large parts even for an insider a black box, which makes exact analysis of the value-added context no easier, as well as a social assessment (think of the potential for discrimination, currently the Berlin initiative d21 initiatived21.de is taking corresponding first steps with the expert group "Algorithms Monitoring"). What is still emerging in medicine as personalised medicine, for example, is for consumers of media an everyday experience (certainly media are far less complex and consequential). Today we see no “MediFy”, but Spotify.
When it comes to trading data (as practised by IQVIA, for example), transparency is less visible. Who really knows how their health insurance provider does the ultimately decisive risk assessment? Which data were used? The fact that you can no longer digitally live without advertising and this advertising is personalised on a data-driven basis, may cost some nerves and evoke countermeasures, such as paying for less advertising; others enjoy hyper-personalised content, but ultimately, it's a comparatively less critical data usage. With patient data selling you will want and have to look more. Opt-out must always be possible for the patient, but today it is not. Just say “No” if you do not want to be part of the game (as long as it is doable for the average person). Solutions such as privacy-enhancing tools, which are available for online offers, for example, are far from available for medical data and records. The data system of the medical and health industry has a breathtaking opacity.
Good providers of data services will ensure transparency and participation, legally offered to patients integrating them economically (and of course doctors, who will soon be seeing new business models in the house, new risks but also new opportunities; no AI will ever replace a good heart (until we do not see an AI as an Existence in the full ethical sense) and doctors are always the natural intelligence needed, think of the actual critical discussion of Watson (IBM). And pay attention to the data quality: statistical modelling is only suitable for intervention in medicine, if it has at least objectivity, reliability and validity with regard to the actual data used and the corresponding analysis methods. With good data, medical systems can be trained and multiple variables can cleverly be linked to newly empirically demonstrable correlations, which in turn may suggest prevention or therapy. Unfortunately, even with data success, neither the corresponding model can be verified nor a causality be proven. Statistics make more or less meaningful predictions depending on the sample size. But that's just what makes new hypotheses possible. And with the exponentially growing flood of information in the medical sector, it's difficult to avoid big data and AI (& Co.). In this sense, in my opinion, patients in the medical and healthcare sector want to deal with their data more sensitively than in previously common consumer areas—and hopefully do it well-informed—and in the end want to use the statistically usable or even personal data-generated value.
On the other hand, what speaks in principle against patients paying in a transparent and well-structured manner, for example, to receive special medical services in a smart hospital with their data? Self-pay may also be achievable for less wealthy patients. What speaks against a patient selling or licensing their genetic data for legal and legitimate and transparent purposes? In the upcoming DNA marketplace, the DNA “donors” should get economic participation; smaller companies such as EncrypGen or Nebula Genomics look for appropriate solutions, and often key technologies such as blockchain play a crucial role. Consequently, questions about the taxation of data will also have to play a bigger role in the future. And, of course, security and economic value issues—hacker attacks from outside and criminal energy within medical institutions—are likely to increase as the incentive potentially increases.
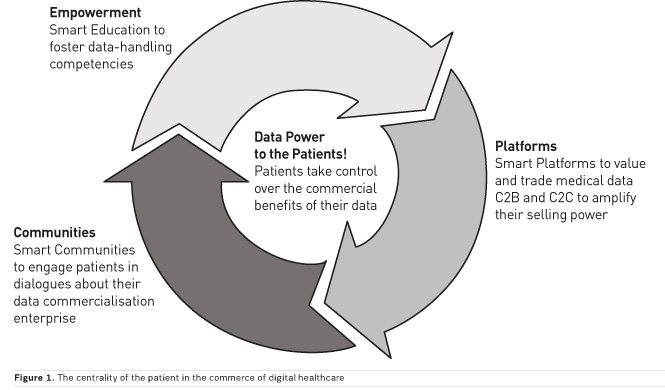
Patients may not have a clear understanding of what their data is really worth, and most of them might not care about the business models at this stage without recognisable participation (in a democratic sense). Companies in the medical and healthcare industry have a decisive advantage here, not least because the value of data constantly changes with the context of (today often unclear, but tomorrow…) business models. Of course, companies are often denied the final clarity on digital business models in the smart healthcare world. In the end, it will be crucial whether patients are adequately involved in certainly-not-marginal welfare gains. Enlightenment is likely to be necessary not only in legal but also in economic terms, otherwise consent declarations remain notoriously ineffective and economically not necessarily positive for the client or patient, because the data-collecting company determines what data it collects for what. But alternatives are also discussed, for instance, personal information management systems (PIMS). Also important are smart communities to engage patients in dialogues about their data commercialisation enterprise among themselves and with medical and other experts.
Not least so that patients not only—as usual in the data economy from the customer's point of view—look for short-term benefits such as discounts or the like, but also take long-term positive effects into focus. This decision-making need not necessarily lead to the decision between added value and the protection of data but can combine both elements. It will not necessarily be about life-changing business when patients use their data or parts of their data economically. But then they are in the game, sitting at the table, and they also should sit there, if, in the end, it comes not through advertising but eg via insurance model-funded data platforms. Patients themselves can increase the price and promote transparency by treating their data with the utmost care, which will be essential for an adequate position of providers (patients) towards buyers (companies). Today it is not foreseeable whether there will be minimal value added, exchangeable, or even a greater value added in the individual economic exploitation of individual, personalised or impersonalised data. A third way to do this would be to point out the current, ultimately unquestioning availability of data and self-marketing of the individual, which is likely to lead to lower prices through asymmetry.
Unlike other consumer data, medical data is absolutely necessary for factual medical care, but for the healthy some medical data are theoretically economically usable even without specific treatment, and not even prevention. The entire life as a prevention and data event is newly articulated in the quantified self. It will probably result in a holistic path connecting electronic medical record (EMR) data, wearables, and business to consumer (B2C)-driven genetic data. A conceivable impact can be the connection between pay and data exploitation, as known and practised in the media industry. The licensing of intangible assets answers the question as to which data, where, when, for how long, to whom and for what purpose and consideration are put into use (Kerber 2016). Companies like to talk about "data ecosystems" as Terminus Technicus instead of "trade". Platforms to value and trade/license C2B and maybe even C2C could be an instrument, but always and only if patients are educated to handle their medical data, which is for example for sure one of the challenges of direct to consumer (DTC) genomic businesses (23andme etc.) because people are confronted with information (might it not be a diagnosis), which they may not be able to handle on their own without further professional advice, eg by a doctor.
In practice, such basically legal issues are not really resolved. In the case of personal data, the term "property", or at least property-like entitlements, may be used, and in the case of non-personal data, it may be called a copyright aspect. Since there are many mergers of data forms that are likely to increase in the internet of things era, even this distinction with property reference may be difficult in practice, and thus the likelihood of lower transaction costs for personal data and its markets. The lawyers will get a lot to do.
If it is ethically correct and legally required in a constitutional state to focus on the patient's benefit, and also economically attractive—albeit a little weird that the patient has to become a customer in order to be a human being with dignity in the health business—then the consistent empowerment of patients to handle their own data is essential. And this does not in the least include the benefit that these can provide—only for the individual patient medically, but also financially, or, for example, by means of data donation in research, potentially for society as a whole or in cooperative models (eg Healthbank in Switzerland). For this, a social consensus must be worked out that supports this form of economic participation. In addition, the lack of factual interoperability of existing patient records is a major obstacle and a significant costly one for convincing implementation. There are initiatives such as MyData from Finland, which generally demand a "human-centred personal data management" for data, and with the concept of the "self-sovereign identity systems" the final idea of the autonomy of users finds its way into the debate. New companies like Longenesis also build on similar approaches.
The GDPR potentially drives the individual data business in medicine
In my opinion, the European Union General Data Protection Regulation (GDPR) tries to manage the balancing act between data protectionism and innovation bondage in favour of a reasonable middle-of-the-range solution. It can, despite certainly not unjustified criticism in detail, become the gold standard to make personal data with privacy and data portability a valuable asset in a seller's market. Businesses, as well as other public-sector institutions, for example, who deal with impersonalised data and, most importantly, personal data of patients, are highly obliged to ensure the maximum possible security of this data from misuse. Since true impersonalised data is not easy to grant, this form of data, although not covered by the GDPR, should be considered data protectio- relevant when we talk about patient data.
It is a good initiative of the GDPR to put consent clearly in the centre. It is about protecting people, not protecting data. In the end, patients will have to learn to responsibly handle the most valuable data they have—their medical data—and to read the privacy policy. The "fine print" re-enters the consciousness, and that's a good thing. In addition, the much-cited informational self-determination is no guarantee of absolute power of the individual over "their" data, because also the protection of privacy takes place in a social context. There remains the problem that the GDPR does not directly address the involvement of consumers in the economic exploitation of their data. It is easy to understand, however, that consumers want more than data protection as soon as the economic opportunities in data markets become clearer to them (Spiekermann and Korunovska 2017). It should be similar for patients, not just because of private return perspectives but also to foster their healthcare outcomes. This might also increase their motivation eg to share their data with research organisations and become a proud data donor. Precision medicine for everyone needs so many institutional barriers to overcome—patients as smart customers can make it happen.
No sensible person can object to better medicine; however, care must be taken to ensure that there are no distorting data monopolies and non-transparent business models that in the end only really benefit a few players. If a legal, legitimate and efficient business is to emerge, it must properly engage patients as customers and data providers in the value chain. The centrality of the patient in the commerce of digital healthcare is crucial—also from my point of view for a holistic patient experience—even though it may be very complex and difficult, it is not impossible.
Key Points
- Data-driven business models make up the medical and healthcare market in large parts, a trend reinforced by further technological developments and regulation. Care must be taken to ensure that, in the end, not only a few big players benefit
- The digital data world is becoming the core of medicine and healthcare
References:
Bourzac K (2016) Participation: power to the patients. Nature 537: 66–8. Available from nature.com/articles/537S66a
Heinemann S (2018) Future medicine, today's healthcare – Is the “Smart Hospital” a chance for change? HealthManagement.org The Journal 18(1): 68–70. Available from iii.hm/j1y
Kerber W (2016) Digital markets, data, and privacy: competition law, consumer law, and data protection. Journal of Intellectual Property Law & Practice 11(11): 856–66.
Lewis A (2018) 13 September 2010. [Tweet] Available from twitter.com/andlewis?lang=en [Accessed 10 August 2018]
Kretschmer T et al. (2018) Datenkapitalismus — eine ökonomische Betrachtung. Wirtschaftsdienst [German National Library of Economics] 98(7): 459-80.
Spiekermann S, Korunovska . (2017) Towards a value theory for personal data; in: Journal of Information Technology 32(1): 62-84.
Sweeney L (2002) k-anonymity: a model for protecting privacy. International Journal on Uncertainty, Fuzziness and Knowledge-based Systems 10(5): 557-70.
