HealthManagement, Volume 21 - Issue 6, 2021
 PRINT OPTIMISED
PRINT OPTIMISED
Key Points
- Prevention, in this context, refers to the condition of the urban environment that prevents the upsurge of specific health problems (clean air with regard to lung health) or facilitates healing (good housing with regard to allergies).
- Health refers to the definition given in 1948 by WHO - “A state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity”.
- Systems theory and systems analysis is the basic approach to study and handle our living environment, in single elements (houses, roads, green area etc.) and when evaluating the interaction among the different elements.
- Complexity theory in this paper is addressed to underline that our existing systems are super connected, and the linear theory based on cause-effect is no longer sufficient to explain the effects that a certain action can produce.
- Determinants of health include a variety of factors which are connected with our physical environment, including quality of water and air, social and economic status, personal habits, good services etc.
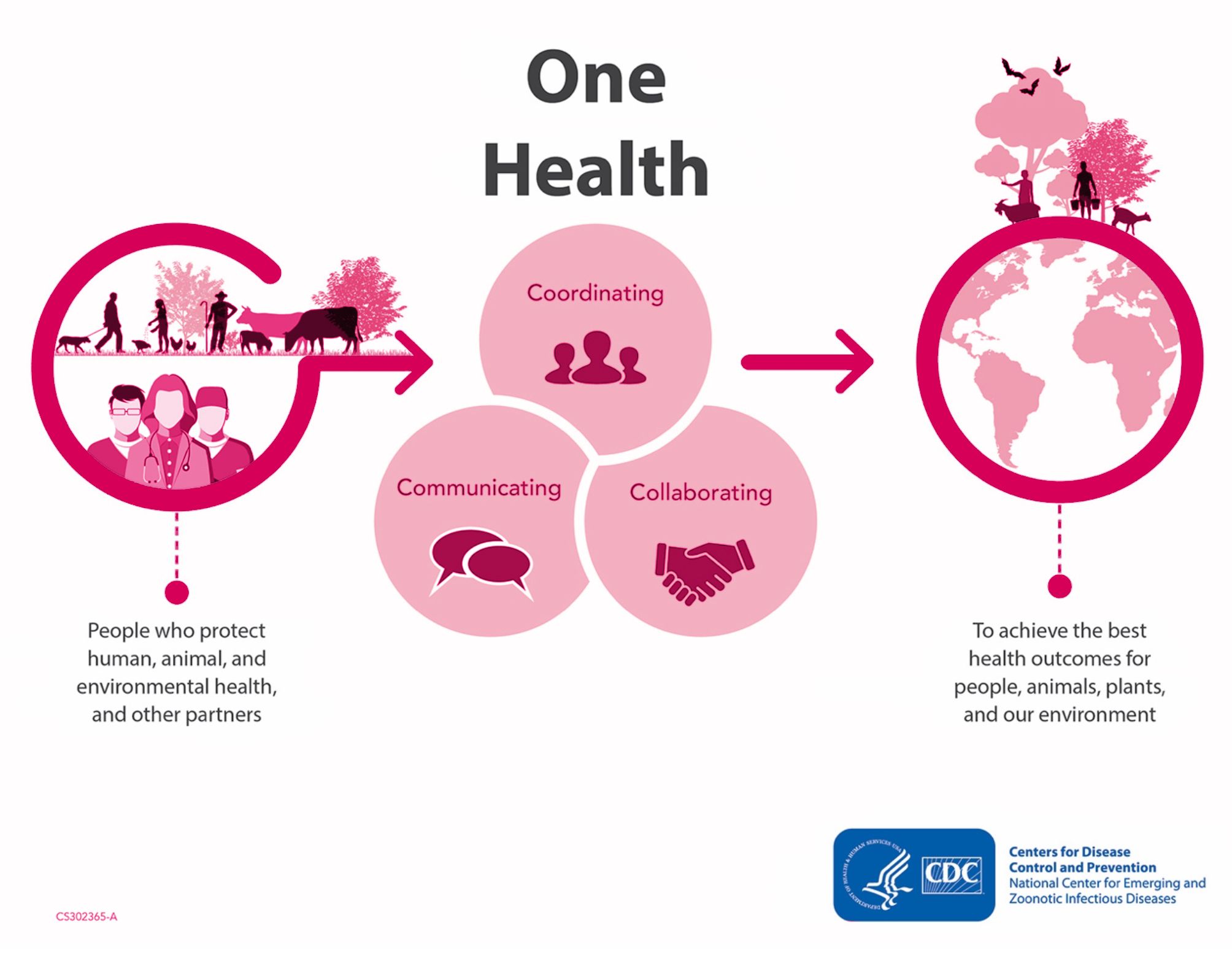
- One Health is a collaborative, multisectoral, and transdisciplinary approach with the goal of achieving optimal health outcomes while recognising the interconnection between people, animals, plants, and their shared environment.
- New Generation –EU (or NG-EU) is the general programme of the EU for helping the economic and social recovery of European countries. Recovery and Resilience Facility (RRF) is the major programme included in NG-EU.
Framework
Urban areas have been at the forefront of the COVID-19 crisis, with 95% of all cases recorded in the first few months in cities. They, consequently, faced a rapidly evolving public health crisis, along with challenges to provide safe public transport and use of public spaces, ensure increased water and sanitation needs, and cope with economic consequences. Many cities in the European Union (EU) had to suffer difficult periods of lockdown amid coronavirus surges.
Apparently, there is a general support for the statement that post-COVID-19 cities cannot return to the “old normal”, but the correspondence with real actions and measures is still to be seen. The challenge of producing the “new normal”, is, certainly, not an easy task and should not be left in the hands of “a few”. The effort of producing this new normal lies in the capacity of choral, cooperative creation of healthy cities and urban environments, based on social equity, inclusion and health support for all. This will have to go in parallel with a much more diffused awareness of the changes that need to be made in comprehending and acting in front of the epochal challenges we are facing.
It is time to take a second look at the assumption that the major agents of change are the city and the healthcare systems. These two elements have to be seen, and dealt with not as two separate organisations, but as complementary entities, having a common point of reference - qualified and measured actions, concretely responding to a “one health approach”.
Let’s go back for a bit to the impact of the pandemic. An overall hasty evaluation of healthcare’s response points out the non-preparedness to this disastrous pandemic. This is attributed to two factors: the inadequacy of the models of health and the shortfall of the urban environment. In other words, the pandemic’s impact has been, on one end, put under necessary scrutiny in terms of handling the assault to health by an exceptional event, and, on the other end, has highlighted the fragility and inadequacy of our everyday living conditions.
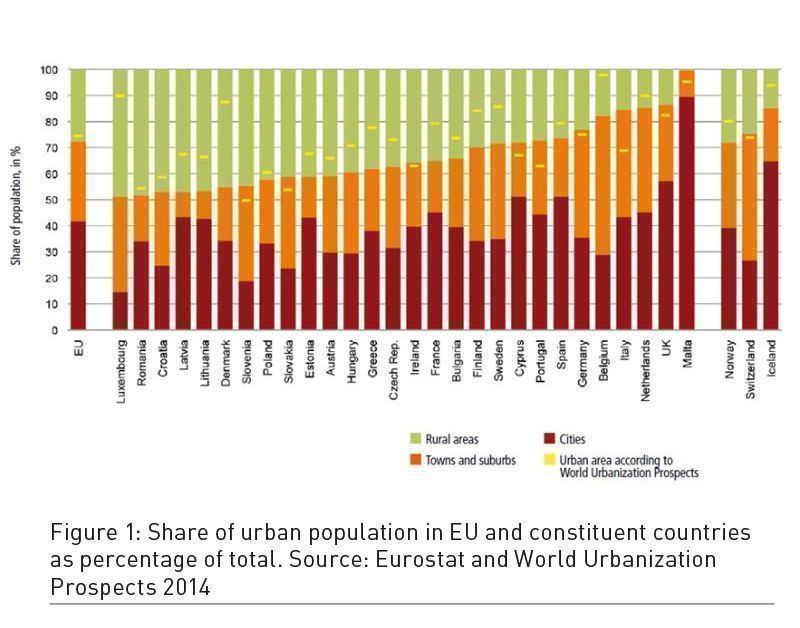
An essay published by the European Development Bank provides data than can put some light on the most recent process of urbanisation of the European continent. “Observing the journeys that European cities have taken from 1970 to 2020 reveal some startling facts. Today, 72% of the EU population lives in cities and urban areas, but this average conceals pronounced differences between countries. Urbanisation rates vary from about 50% (Luxembourg, Romania, Croatia) to beyond 80% (Italy, Netherlands, UK) … by most definitions, Europe has no megacity. There is no single municipal area with more than 10 million people. But the wider city-regions of London, Paris, and Milan each have more than 10 million”. Size is certainly playing a role and there are several other large cities in Europe with a consistent urban sprawl, with degraded areas in unplanned expansions, but sometime urban decay and poor living conditions are present also in historic centres. Furthermore, as we said, expansion took place in many cities of Europe after World War II. This expansion occurred mainly under the banner of private building speculation, or, to speculate bluntly, mostly according to criteria, models and standards in which the economic values of the land were prevalent and profit was the primary goal. The public governance, in many cases, lacked economic means and effective legal tools for controlling the development. Most of the local authorities, elected to manage public affairs, lacked a true awareness that urban policies could influence the quality of air, space and water, the common use of public space, and access to essential services. This facilitated the insurgence of some diseases and the diffusion of others.
Today there is more advanced knowledge and awareness of the consequences of urban policies and decision making on the environment, the psycho-physical health of urban people, and on the quality of urban life. This has additional relevance since the trend of growth is expected to be around 90% in Europe.
Public health management and urban planning policymakers have operated separately in a neoliberal framework within academic, political and strategic compartments, representing one of the important obstacles, rarely mentioned, for moving towards a “new normal”, as we will illustrate, digging into the parameters that could potentially make this possible.
First Steps Along the Journey Toward Change
As underlined before, the need for a post-pandemic “new normal”, in other terms for change, is recognised, or should be recognised, as regarding the two “organisms” on which we have focused: the city and the healthcare systems. We consider that there will be no change unless a few important aspects are bilaterally understood. These include:
Prevention
It is well understood and accepted that the health of people is not only a matter of medicine, and therefore, does not completely fall under the responsibility of health systems. This is especially true if we look at the 1948 definition of health by the World Health Organization (WHO). The definition today has become more and more diffused. This has been expressed quite eloquently by the title of Nagel Krisp’s last book - “Health is made at home, hospitals are for repair”, echoed by Prof Rafael Grossman proposing to change healthcare into health repair.
There is some truth in this, considering that medical doctors themselves indicate that medicine, including care in hospitals, covers no more 15-20% of the average health needs of a person during his lifetime. A large majority of the medical doctors and scientists stress that a part of medicine should be dedicated to preventing illnesses. Other important scholars have also put the current approach of many European countries under scrutiny in terms of how prevention is conceived and practiced and why there is a need to change the concentration on “diagnosis and care” as the way to prevent diseases.
Saracci et al. (2021) in a recent article stress that the pandemic has given evidence that such systems are obsolete and there is a need for new parameters. They also stress on “the policy of co-benefits”. As an example, they indicate that interventions aiming to the reduction of greenhouse gases (GHG), through reducing the use of fossil fuels will jointly prevent diseases induced by air pollution and those induced by climate change.
This is an important aspect and gives a more interesting perspective on how a hospital needs to come out of its isolation. Analysis of the impact of the COVID-19 pandemic, as mentioned before, has brought attention to the fact that there was not enough presence of health infrastructures in most global territories. This is correct, but not enough.
Focusing on improving the infrastructure according to quantitative parameters is a positive change and could bring healthcare systems closer to the needs of patients, but this will still not be part of the real prevention that can come from a city, that, with the collaboration of healthcare, can generate larger co-benefits.
Another factor is the pressure for improving the quality of housing. For example, taking care of asthmatic children in a hospital knowing that, once home, these children would become sick again due to the poor living conditions. This is currently not considered a problem of the hospital and this, in itself, indicates how much space there still is in establishing a common understanding between hospital and city government based on the policy of co-benefits.
During these times, when urban planning tools are under re-evaluation, it has become essential that a priority alliance between healthcare and urban governance gets established to focus on a common understanding of the definition of prevention and elaboration of a common strategy to help the urban environment become, as I have defined in another article, the gym for health. The “policy of co-benefits” already mentioned is certainly an important tool.
Even before the pandemic, WHO in its Global NCD (Non Communicable Diseases) Action Plan 2013-2020 recognised the primary role and responsibility of the government and highlighted the importance of urban planning related to life conditions and environment. The document also emphasises another important point: urban policies and healthcare governance are among the main determinants of prevention, but involvement and actions have to extend to a transdisciplinary participation, and they have to be oriented by the principle of “health in all policies”.
Complexity and Systems Approach
Scholars and urban theorists have, for a long time, conceived that in the field of urban planning and policymaking, the approach had to be “rational” positivist, based on objective data, deductive analysis, and systematic comparison of alternatives. In recent times and especially with the pandemic experience, this approach now feels obsolete. In fact, since the pandemic started to intrude and upset our lives, we have had to recognise that we live in a world characterised by multiple connections, with continuous variations which don’t obey to the linear thinking based on cause and effect – a concept that has constituted the basis of our thinking for many centuries.
“A new way of thinking is becoming imperative because the systems in which we live, urban and environmental and biological, social, financial and economical, to mention some of the most relevant, don’t follow linear logics of cause and effect. Given the high presence of non-linear relationships, in complex systems the effect of a stimulus is not proportional to the force that generated it ” writes Antonio Bonaldi (2020).
Recognising the complex nature of urban policies and healthcare organisation and delivery of health services, obliges us to also look at the common ground of prevention and the need for a new way of thinking and new approaches. The fundamental of this has been constituted by the Systems Approach. It represents, in fact, the support in understanding and building the transdisciplinary relationship involved in reaching the goals related to a health-protective urban environment and a healthcare system that is a pro-active participant in its realisation.
To make more concrete the understanding of what would work within the framework of the systems approach, here is a small example. Reopening schools safely has been and still is, a matter of debate - from politicians to parents - not only in Europe but around the world. In effect, the first attempt of reopening schools was focused on life inside the schools (e.g. changing school desks or chairs, sanitisation etc.). But this proved to be a great failure. Only recently, many of the previously non-considered dimensions, such as transportation of children/young students, safety measures for teachers and all other people involved in school life and activities, family organisation etc. are now being taken into consideration, that will hopefully produce the desired result.
Certainly, the Systems Approach is necessary in understanding more complex problems such as the way to build healthy cities also depends on the need to limit the increase of the effects of climate warming and climate change. It is a systemic view that is advocated, among others, by Richard Heinberg in his many books and articles highlighting the profound links between ecological problems and the way human society acts.
It needs also to be said that systems analysis is not a new discipline. An explosion of systemic research, started by Jay Forrester with his “Urban Dynamics” produced way back in the 70’s and the work of Club of Rome with M.I.T. “The limit of Growth” highlighted the relationship between growth of the population, industrial production, food production, depletion of natural resources, and pollution. It may be worth it to rediscover that period, without the superficial use and abuse of the reference to systemic approach. This leads us to another important concept that needs less superficial attention.
One Health
The One Health approach seems a very easy concept to grasp and use. In reality it isn’t so. Let’s take one of the many definitions proposed by the Centre for Control of Diseases and Prevention (CDC): “One Health is a collaborative, multisectoral, and transdisciplinary approach — working at the local, regional, national, and global levels — with the goal of achieving optimal health outcomes recognising the interconnection between people, animals, plants, and their shared environment”.
As mentioned before, there is at least one serious ancestor of this concept. It was the attempt by the European Union to introduce the health factor into the different sectorial policies of EU. Working on the high level committee in Brussels,
I remember the complicated cube we produced to provide a tool to ensure that EU policies were having a positive impact on health or, at least, were not inducing consequential
health problems.
Our work did not go as far as it should have gone. WHO took it further, however, in 2013- 2014 when it produced a document defining five key elements of a “Health in All Policies Approach” (WHO 2014):
- Health, equity and sustainability. The Health in All Policies philosophy holds that health, equity and sustainability are closely linked
- Intersectoral collaboration
- Co-benefits: Benefit multiple partners
- Engaging stakeholders
- Creating structural or procedural change
What appears from these brief references is that “One Health” represents the evolution of a concept with a very big step forward created by the consciousness of “one planet, one health” - that is human health cannot be separate from animal and environment health.
To give concreteness and impact capacity to this concept is a battle certainly not yet won. Some tools have to be created, even at the risk of excess of bureaucratisation, and in any case, the results for a new normality will not be achieved without massive people involvement.
The Italian First Steps Toward Recovery and Resilience: A Case Study
The presentation of this very recent planning action by the Italian government aims to reinforce the concept already expressed: change is difficult and with it the realisation of a “new normal”. The “Next Generation EU” (NGEU) is the well known European plan for Recovery and Resilience. This is a unique effort made by European institutions to help EU countries recuperate after the crisis produced by the pandemic. Recovery and Resilience Facilities (RRF) is the most important of the programmes financed by NGEU.
We will analyse some of the aspects of PNRR (National Plan for Recovery and Resilience) - the Italian plan that has an allocation of 191,5 million Euros. The reason for the selection of this plan is because documentation for Italy is available to the writer. The complementary assumption is that difficulties and the risks facing Italy would have, in large part, similarities with several other EU countries.
The regulation lines of the RRF indicate six pillars as the focus for each national plan. These include:
- Green transition
- Digital transformation
- Intelligent, sustainable and inclusive growth
- Social and territorial inclusion
- Health, economic, social and institutional resilience
- Policies for new generation, childhood and youth.
The Italian plan has divided the resources in sixteen parts, called components, grouped in six missions. One of these missions is dedicated to health. The first critical evaluation comes from comparing how pillar five is defined by the EU-RRF compared with the Italian setting. In the latter, HEALTH is defined in reductive terms. The reference is only to some sectors of health assistance. In the EU guidelines, “health and consequently all what contributes to determine health, has to be privileged, being influent on the growth capacity of the states to grow.” In the Italian document, health is considered only in reference to some limited aspects of the healthcare organisation”. This point has also been highlighted in the article by Saracci et al. (2021).
The role of territorial assistance appears to be one of the weak points in the protection against the impact of the virus It is again seen as part of the health infrastructure, not an occasion of integration within the social fabric and an element to build a common vision between health policymakers and local governments. This is certainly a confirmation that there is no real vision that should take us towards the “new post-pandemic normal”.
There is a total absence of any reference to “prevention”, the importance of which has been highlighted at length both for the city and the healthcare system, and which is critical for working together. Another lesson that can be derived from the Italian PNRR is that although the One Health Approach is frequently mentioned, it is not put into practice. A real understanding of its value would have certainly induced to see health involved in many, if not all the other missions, from mission 2 to mission 5. However, health is mentioned only in mission 1, and that too, related to digitalisation of medical records. Furthermore every action outlined in the components of the missions written in the PNRR are examined based on their impact on the economy. They should also be critically examined with regard to the favourable or negative impact on health, but this would only happen if the One Health Approach should have been concretely understood and made an important part of its initiatives.
Conclusion
We have at length, expressed our concern that the great occasion for change will not become a reality, or even if it does, it will produce low results. Getting back explicitly to the question of the present issue of HealthManagement.org, we are certainly in a period of great challenges and opportunities for change. We have the opportunity to produce healthy cities thanks to the collaboration of local governments and communities with a healthcare system, public mostly, but also private, to integrate prevention and use of the criteria of co-benefits as a different view of care. At the moment the efforts don’t seem to encourage optimism. We must, however, concede that to make plans operative, we will require plenty more studies and definitions, which can address omissions and some wrong visions and approaches. For Italy, a comparison with other countries will certainly be of great help. Globally, it will help the diffusion of new visions and concepts, including the ones we have discussed in this article.
Conflict of Interest
None.
References:
Bonaldi A (2020) Towards the Ecology of Health. Available from www.wsimag.com/scienza e tecnologia/63037.verso-unecologia-della-salute
Forrester JW (1969) Urban Dynamics. Pegasus Communications Inc.
Meadows DH, Meadows DL, Randers J, Behrens WW III (1972) The Limits to Growth. Universe Books, New York.
One Health. CDC. Available from https://www.cdc.gov/onehealth/index.html
Recovery plan for Europe. European Commission. Available from https://ec.europa.eu/info/strategy/recovery-plan-europe_en
Saracci R, Forastiere F, Vineis P (2021) Where is the prevention in the National Recovery and Resilience Plan? Scienzainrete. Available from https://www.scienzainrete.it/autori/saracci/2333
The Story of Your City: Europe and its Urban Development, 1970 to 2020. (2018) European Investment Bank. Available from https://www.eib.org/en/essays/the-story-of-your-city
What you need to know about health policies. World Health Organization. Available from https://www.who.int/social_determinants/publications/health-policies-manual/key-messages-en.pdf
WHO Constitution. World Health Organization. Available from https://www.who.int/about/governance/constitution
