HealthManagement, Volume 17 - Issue 3, 2017
 PRINT OPTIMISED
PRINT OPTIMISED
With chest pain a leading reason for an emergency room visit, what is new in training and recertification processes for chest pain units?
The chest pain syndrome remains a single leading cause for contacting an emergency unit (Hollander, et al. 2016). Chest pain units (CPU) are specialised units in the emergency room that handle patients with all forms of acute chest pain and discomfort. Beginning in 2008, the German Cardiac Society has outlined the minimum standards that certified CPUs must comply with. These guidelines were updated in 2015 and also refer to the recertification/ reaccreditation process for previously-certified centres (Post et al. 2015). These specific criteria relate to the training of the medical personnel, the required diagnostic tools, the timing of the diagnosis process including laboratory testing, and the transfer of patients to the catheter laboratory or intensive care medicine units. The foremost goal of the certification process is to provide a standard of care throughout the country for the management of acute chest pain and to comply with the guidelines for the management of acute coronary syndromes (unstable angina, non-ST elevation myocardial infarction [NSTE MI], and STE MI).
Large cohort studies have demonstrated that patients with undiagnosed or poorly-diagnosed causes for chest pain at primary presentation are under an incremental risk for cardiovascular events in the next years (Jordan et al. 2017). The implementation of a unified standard of care including diagnostic algorithms and treatment pathways is therefore compulsory for the optimal treatment of patients as well as for the reduction of costs. In this context, the continuous evaluation of CPUs as and the recertification process therefore allow for a precise statistical evaluation of the care quality. In this article, we outline the hallmarks of a CPU in relation to personnel/teaching, diagnostic tools and pathways, infrastructure and therapeutic pathways. Finally, we will comment on the recertification process.
Personnel
The CPU is implemented in a clinic for cardiology; the supervising physician has to be board-certified for internal medicine and cardiology. Trained medical personnel must be present and a board-certified cardiologist must be available at any time. The training requirements for chest pain unit physicians particularly refer to the diagnostic skills in emergency echocardiography and resuscitation including intubation etc. (Post et al. 2015). Although not required, however in our opinion CPU physicians should be trained in emergency echocardiography as well as in emergency ultrasound particularly for the vasculature. These skills are complemented by assessment of pacemakers and extended ECG interpretation. In order to train and teach emergency algorithms it is furthermore necessary to conduct weekly team sessions to provide the usually large team with the necessary up-to-date knowledge. This includes special sessions for life support trainings (BLS, ALS) by certified instructors. Moreover, we conduct regular morbidity and mortality conferences in order to re-assess particular cases. In order to provide optimal CPU care, it is therefore critical to provide a teaching programme for each individual physician and for the whole team. Finally, the medical programme in a CPU must be closely connected to the intensive care department, the resuscitation team and the catheter laboratory.
Infrastructure
The CPU can be located in the cardiology department or can be implemented in a general emergency room environment. At least four monitoring units must be provided.
However, given the current patient numbers in most CPUs, six
to eight monitor beds will be required at most centres. At a rule, one bed per
50,000 inhabitants should be provided. It should be advised that at least some
of the monitor beds can be used for patients with multi-resistant bacterial
colonisation. The CPU must be in close distance to the catheter laboratory, the
radiology department (X-ray and computertomography) and the intensive care
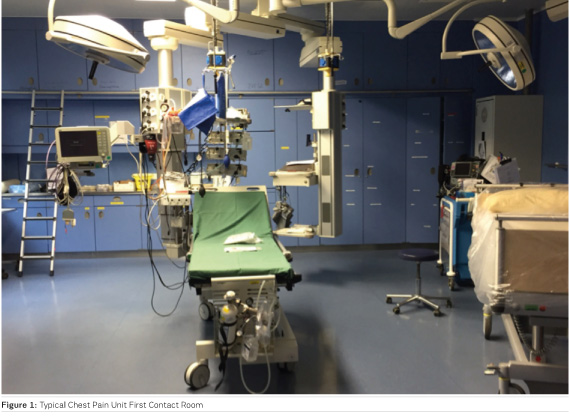
department (all within minutes). The following diagnostic tools must be
immediately available (Figure 1): ECG, transthoracic and transoesophageal
echocardiography, resuscitation devices (intubation, defibrillator), and
transport units (perfusor, oxygen, respirator).
You might also like:AI in Precision Cardiovascular Medicine
Diagnostic Approach
Every patient with chest pain is assessed by a physician together with a blood test and an initial ECG (12-channel standard ECG, posterior leads V7-V9 and the right precordial leads). The results for cardiac enzymes (high sensitive troponin) must be available within 45-60 minutes and can be complemented by point-of-care testing. This is followed by an assessment of the c ardiovascular history/symptoms a nd a complete clinical examination. A second testing after three hours (for high sensitive troponin) must be performed for all patients with pain lasting shorter than six hours. The results can be summarised in clinical scoring system, e.g. the GRA CE score using eight parameters (e.g. age, heart rate, ST -segment deviations). This will help to determine at what time interval (immediately, within two hours, within 24 or 72 hours) a patient will have to be transferred to the catheter laboratory. We have established a control system at our CPU particularly for the blood test results. After blood taking, the nurse/physician confirms that blood samples are readily transferred to the central core laboratory. Results are transmitted by telephone to the physician on call and timing is registered for every sample. We have furthermore developed a one-page CPU report including all relevant results for each patient (cardiac enzymes, symptoms, echoparameters, X-ray results, GRA CE score). Following this initial assessment, the patient is either dismissed with referral for non-invasive stress testing within one to three days or treated according to the standard therapeutic algorithms that should be available in the CPU and to the complete staff. The German Cardiac Society requires therapeutic pathways for acute coronary syndromes, rhythm disorders, pacemaker/ICD malfunctioning, pulmonary embolism, aortic syndromes, heart failure, hypertensive emergencies, resuscitation, prevention and syncope.
The Recertification Process
This process follows the identical rules set out for first-time CPU evaluations. After a formal proposal to the German Cardiac Society, the CPU is evaluated by the society by local visitation. This includes the infrastructure as well as a reassessment of the required timing (laboratory testing), personnel skills and certifications, regular team meetings and morbidity and mortality conferences and the therapeutic algorithms. The process is finished if all requirements are fulfilled. In our opinion, this procedure significantly improves the care for chest pain patients as it automatically provides standardisation for the diagnostic and therapeutic procedures throughout the country. This also requires cardiology departments to re-evaluate their infrastructure continuously and to reassess the interrelation with the resuscitation team, the radiology department, the catheter laboratory and intensive care unit. Adherence to guidelines in certified CPUs (Breuckmann et al. 2016a; Breuckmann et al. 2016b) significantly improves the outcome for acute chest pain patients (Varnavas et al. 2017). Particular attention must be directed to adequate scoring and risk profiling of troponin-negative and positive ACS patients in order to ensure the guideline-conforming care.
References:
Breuckmann F, Remberg F, Bose D, Waltenberger J, Fischer D, Rassaf T. (2016) On-versus off-hour care for patients with non-ST-segment elevation myocardial infarction in Germany: Exemplary results within the chest pain unit concept. Herz. Dec;41(8):725- 31. PubMed PMID: 27193907. Timing der invasiven Koronardiagnostik bei NSTEMI-Patienten in der Chest-Pain-Unit : Exemplarischer Vergleich von Regelarbeits- und Bereitschaftsdienstzeit.
Breuckmann F, Rassaf T. (2016) First Update of the Criteria for Certification of Chest Pain Units in Germany: Facelift or New Model? Critical pathways in cardiology. Mar;15(1):29-31. PubMed PMID: 26881818.
Hollander JE, Than M, Mueller C. (2016) State-of-the-Art Evaluation of Emergency Department Patients Presenting With Potential Acute Coronary Syndromes. Circulation. Aug 16;134(7):547-64. PubMed PMID: 27528647.
Jordan KP, Timmis A, Croft P, van der Windt DA, Denaxas S, Gonzalez- Izquierdo A, et al. (2017) Prognosis of undiagnosed chest pain: linked electronic health record cohort study. BMJ. Apr 03;357:j1194. PubMed PMID: 28373173. Pubmed Central PMCID: 5482346.
Post F, Giannitsis E, Darius H, Baldus S, Hamm CW, Hambrecht R, et al. (2015) Kriterien der Deutschen Gesellschaft für Kardiologie - Herzund Kreislaufforschung für "Chest Pain Units". Kardiologe; 9:171-81. Epub 27.02.2015.
Varnavas V, Rassaf T, Breuckmann F. (2017) Nationwide but still inhomogeneous distribution of certified chest pain units across Germany: Need to strengthen rural regions. Herz. Jan 23. PubMed PMID: 28116466.

