




ICU Management & Practice, Volume 16 - Issue 2, 2016
 PRINT OPTIMISED
PRINT OPTIMISED
Technological advancement has made robots an integral part of several fields, including medicine. This article provides an overview of the application of robots to anaesthesia, highlighting recent developments. Pharmacological robots are closed-loop systems, able to precisely titrate the dose of anaesthetic drugs to a preset value, concerning hypnosis, analgesia and neuromuscular block. New evidence shows the possibility to feasibly control haemodynamic, respiratory and metabolic parameters. Mechanical robots automatically reproduce manual tasks, showing promising performance. Decision support systems and teleanaesthesia can improve clinical practice. The use of robots in anaesthesia shows the advantage of eliminating the repetitive part of the workload, allowing the anaesthesiologist to focus on patients. Additional studies will be addressed to test safety and refine algorithms of functioning, in order to maintain homeostasis through an automatic integrated control of all biological variables.
Background: the Rationale for Robots in Anaesthesia
The use of robots is part of the technological advancement in several aspects of our lives, from aviation to construction, from industry to medicine. Different definitions of robots have been presented (Hemmerling et al. 2011a). Automation, reproducibility and precision of an action are key elements of robots, which make their use advantageous. Recently this progress has involved the field of anaesthesia. The concepts of robotisation and automation have a potentially great impact on anaesthesia for different reasons. Essentially robots perform measurements, make decisions and perform actions accordingly, which represent what anaesthesiologists continuously do to maintain body homeostasis (Dumont and Ansermino 2013). The activity of anaesthesiologists is displayed in complex environments (operating room, intensive care unit) and requires technical and non-technical skills to be competently implemented (Smith and Greaves 2010). The repetitive implementation of technical and nontechnical tasks (e.g., manual tasks, decisionmaking) during the day, or even in an emergency, may negatively affect the performance of further tasks, due to the accumulation of fatigue and drop in alertness, factors exacerbated by ageing and possible coexisting issues, with a variable safety outcome for patients (Atchabahian and Hemmerling 2014). Robots can eliminate the repetitive part of the workload, the acquisition of patient data, decision-making and manual tasks, and allow anaesthesiologists to efficiently focus on patients and the related perioperative issues (Cannesson and Rinehart 2014). Consequently, the workload is ‘smartly' distributed and implemented as if the anaesthesiologist had a technological mental and physical ‘extension’. In addition, several physiologic functions can be seen as a combination of automatic feedback circuitries, which can be controlled by robots in such terms. This change would mean the increase in accuracy and safety of the care being delivered, with robots assisting this process without replacing the conduct of anaesthesiologists. For these reasons, two main types of robots have been developed in anaesthesia: pharmacological robots and mechanical (or manual) robots (Hemmerling and Terrasini 2012). A third category is represented by decision support systems: they can be regarded as precursors of robots by helping anaesthesiologists in decision-making through relevant and updated information. This article will present an overview on the application of robotisation in anaesthesia, focusing on the latest advances.
Pharmacological Robots
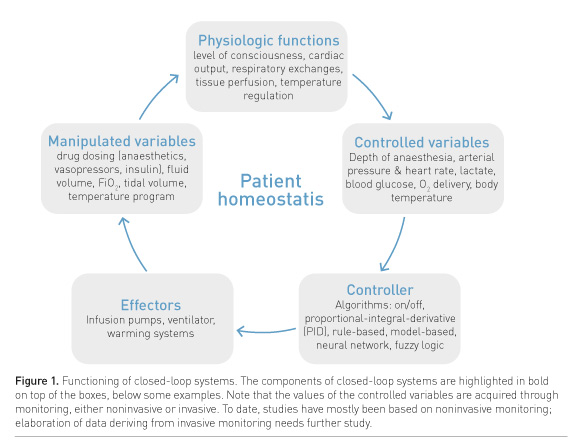
Pharmacological robots are designed to correctly titrate anaesthetic drugs (Hemmerling and Terrasini 2012) and control biological parameters of anaesthetic concern. Robots exert a control, meaning the regulation of the functioning of a system in drug administration (Dumont and Ansermino 2013), which is performed by a closed-loop modality. Closed-loop or feedback control means that in predetermined time intervals a controller acquires measurements of a variable (controlled), which are compared to a desired target value (set point): if there is a difference, the controller modifies the manipulated variable in order to restore the controlled variable to the set point (Dumont and Ansermino 2013). On the basis of this model, three main elements are recognised: software (the controller), an effector (e.g., drug delivery system, ventilator) and some variables (usually one controlled and one manipulated, deriving from either the patient or the effector). Robots continuously adjust the administration of drugs and maintain a biological target without manual input (Hemmerling and Terrasini 2012). To date the closed-loop control has been applied to the three components of anaesthesia: hypnosis, analgesia and neuromuscular block. Recently, new applications concerning ventilation, haemodynamic homeostasis, metabolism and temperature have been developed (Dumont and Ansermino 2013). These modern additions may allow anaesthesiologists to have complete feedback control of all aspects of human homeostasis (Fig. 1).
Management of General Anaesthesia
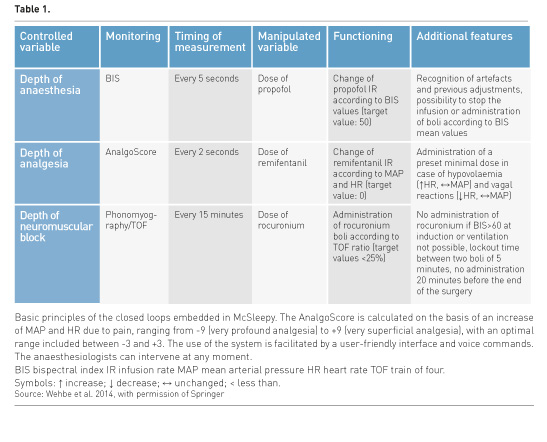
The idea of automation in anaesthesia is not new. The first trials date back to the 1950s when volatile anaesthetics were automatically administered using the electroencephalogram (EEG) (Bickford 1950). Schematically the relatively few works which followed were carried out on volatile anaesthetics using the EEG as input variable or on neuromuscular block. Limitations in the availability of means for monitoring, the advancement of systems for controlling (software), as well as the development of intravenous anaesthesia explain the initial slow development of automation. An important step was the introduction of the Bispectral Index (BIS) to objectively measure the depth of anaesthesia. The BIS was initially applied to isoflurane (Gentilini et al. 2001) or propofol general anaesthesia (Absalom and Kenny 2003). The closed loop was used for maintenance only in both cases, controlled by computer software. Other attempts at automation of anaesthesia were made, with more refined systems for control. A closed-loop anaesthesia delivery system (CLADS) has been successfully used for both induction and maintenance of total intravenous anaesthesia (TIVA), by intervening on the hypnotic component only (single loop) (Puri et al. 2007). The target BIS value was set at 50 and measurements were acquired every five seconds; the control algorithm adjusted propofol infusion according to these measurements and the last adjustments of dosing: the overall quantities of propofol were significantly lower in patients followed with CLADS than controls and these patients had a quicker recovery (Puri et al.2007). This system was shown to function also in difficult environments, such as high altitude (Puri et al. 2012). A new closed-loop system for propofol administration was demonstrated to perform better than manual administration (Hemmerling et al. 2010a). It has an adaptive, rule-based algorithm, meaning that the administration takes into account a set of rules applied to modify the drug dose to achieve the target effect. These rules include different factors, i.e., previous adjustments, BIS trend, BIS artefacts, maximum and minimum allowance of dosing, etc. (Hemmerling et al. 2010a). In another study (Liu et al. 2011) BIS monitoring was applied to the control of the administration of both propofol and remifentanil. Due to the presence of two manipulated variables (dose of two drugs), the system is acknowledged to be dual loop, even if the controlled variable (depth of anaesthesia) is one, based on the assumption that painful operative stimuli cause cortical activation reflected by a reduction of the depth of hypnosis and analgesia and consequent increase of BIS. The control of hypnosis and analgesia was acceptable, with quicker extubation (Liu et al. 2011). This dual loop system was further refined by using the M-Entropy (GE Healthcare, Milwaukee, WI, USA) as monitoring: similar to BIS, it is derived from EEG and elaborates two components, state and response entropy, one for hypnosis and one for analgesia, respectively (Liu et al. 2012). The management of general anaesthesia was better than expert manual control (Liu et al. 2012). A new system called McSleepy was introduced as a pharmacological robot able to autonomously control hypnosis, analgesia and neuromuscular block at the same time, in regard to induction, maintenance and emergence (Hemmerling et al. 2010b). Each variable has specific monitoring (BIS, AnalgoScore and train of four [TOF] phonomyography, respectively) (Table 1). Total intravenous anaesthesia was successfully administered to 30 adult patients by McSleepy (Hemmerling et al. 2010b). Significantly more time with excellent control of hypnosis and good control of analgesia was obtained in comparison to the control group. A trial on a larger number of patients (185 overall) confirmed these data, showing a performance better than manual administration (Hemmerling et al. 2013a). McSleepy has some additional and safety features which make it a real robot for anaesthesia (Table 1) (Wehbe et al. 2014). The control of anaesthesia provided by McSleepy can be bypassed by the anaesthesiologist when needed (Wehbe et al. 2014). Other research has used monitoring other than BIS (NeuroSENSE Monitor (NeuroWave Systems Inc, Cleveland Heights, OH, USA) to administer propofol for general anaesthesia in closed loop (Dumont et al. 2011). This has been safely and effectively applied to the delivery of general anaesthesia to children, for both induction and maintenance, using appropriate kinetic and dynamic models (West et al. 2013). Recently, systems integrated into the anaesthesia workstation have been introduced to automatically adjust the fresh flow gas and the inspired concentration of inhaled anaesthetics to reach a set value of expired concentration (Singaravelu and Barclay 2013). A new trend is emerging in regard to closed-loop anaesthesia, which is the possibility to simulate the administration of anaesthetic drugs (in silico simulations). Computerised models have been developed to simulate patients and test closed-loop control of intravenous drugs, increasing the safety of the real administration (Fang et al. 2014; Liberman et al. 2013). This is now possible also for volatile anaesthetics, allowing a significant reduction of dosing by applying a low fresh gas flow (Luria et al. 2013). In addition, based on the precision of dosing, the use of closed-loop systems, unlike manual administration, allows performance of fine evaluations of the potency of drugs, for instance the comparison among three commercially available formulations of propofol (Le Guen et al. 2014). Recently the application of closed-loop systems has been extended to other components of the practice of anaesthesia. In a population of preterm infants receiving either invasive or noninvasive respiratory support and supplemental oxygen, the manual control of the inspired fraction of oxygen (FiO2) was compared to the closed-loop control: with the closed loop, the percentage of time with the target arterial oxygen saturation was significantly higher than that with the manual control, achieving a reduced need for adjustments of FiO2, even if not significant, and so a reduced repetitive workload (Hallenberger et al. 2014). Despite the current absence of compelling evidence, studies are being carried out to apply closed-loop systems to the control of mechanical ventilation and the performance of spontaneous breathing trials for weaning in adults (Burns et al. 2014). The development of noninvasive and refined means of haemodynamic monitoring as well as the superiority of goal-directed fluid therapy has also led to automation in these fields. A recent in silico study (Rinehart et al. 2012) shows that closed-loop systems for fluid resuscitation are effective in the maintenance of cardiac output, stroke volume and arterial pressure to the targets, detecting the need for fluid adjustments and vasopressors before anaesthesiologists, with fewer variations, and working well regardless of weight, heart contractility and initial volaemic state (Rinehart et al. 2013a). An in vivo study in pigs confirms these results (Rinehart et al. 2013b). For humans, closed-loop control of vasopressors (ephedrine and phenylephrine) was shown to perform better than manual control of hypotension in patients undergoing caesarean section under spinal anaesthesia (Sng et al. 2014). Closed-loop systems are also effective for controlling glycaemic levels in critically ill simulated patients by adjusting the insulin delivery rate without significant fluctuations (Wang et al. 2014).
Management of Sedation
Sedasys® (Ethicon, Somerville, NJ, USA) is a computer-assisted personalised system intended for mild to moderate propofol sedation in healthy adults, managed by a non-anaesthetist member of staff (Banerjee et al. 2011). This device has been approved in Canada for colonoscopy (Banerjee et al. 2011) and in Australia, the European Union and the United States for colonoscopy and oesophagogastroduodenoscopy (Banerjee et al. 2011; Goudra et al. 2014). The system records patient data (e.g. arterial pressure, saturation, respiratory rate), automatically adjusts propofol rate infusion, oxygen flow and also gives cues to optimise patient responsiveness (Banerjee et al. 2011). Another system is the hybrid closed-loop sedation system (HSS), defined as hybrid since it includes a decision support system and a closed-loop control for propofol administration (Hemmerling et al. 2011b; Zaouter et al. 2016). It was tested in patients undergoing hip or knee arthroplasty under spinal anaesthesia and propofol sedation, monitored by the BIS. In the HSS group, the control of sedation showed more consistency and the control of adverse events (apnoea, hypotension) was more accurate than manual control (Hemmerling et al. 2011b).
Mechanical Robots
This kind of robot is designed to give support or replace manual gestures of anaesthesiologists. The two main fields of application are endotracheal intubation and regional anaesthesia. In regard to intubation, a first trial involved the use of the da Vinci® Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA, USA) in the performance of two simulated fibreoptic intubations, which were both successful even if technically difficult due to the robot design with multiple robotic arms (Tighe et al. 2010). The Kepler Intubation System (KIS) (Hemmerling et al. 2012a) is composed of one robotic arm linked to a standard videolaryngoscope at one end, and remotely controlled by a joystick controlled in turn by a specific software and interface (Fig. 2). Intubations can be performed automatically or semiautomatically, under direct vision or remotely: procedural time ranged overall from 40 to 60 seconds in 90 simulated intubations, which were successful at the first attempt (Hemmerling et al. 2012a). In a trial in 12 patients, the KIS showed a success rate of 91% with a mean procedural time of 93 seconds, without complications (Hemmerling et al. 2012b). In regard to regional anaesthesia, an attempt at ultrasound-guided nerve block and placement of a perineural catheter was carried out on a phantom using the DaVinci System, with the same constraints mentioned for intubations (Tighe et al. 2010). The Magellan system (Oceanic Medical Products, Inc., Atchison, KS, USA), has been developed to perform robotassisted, ultrasound-guided nerve blocks by the use of a robotic arm, with a nerve block needle at the end, guided by a joystick and controlled by a specific software and interface (Fig. 3) (Tighe et al. 2013). A success rate of 100% was achieved on a standard ultrasound phantom (Tighe et al. 2013) and subsequently in 13 patients undergoing popliteal block with a maximum procedural time of 4 minutes (Hemmerling et al. 2013b). This system could be integrated with software which allows for the automatic recognition of the nerve on the ultrasound image, without human search (Wehbe et al. 2012). It is still under development after the first promising results (Wehbe et al. 2012). In addition, it has been recently shown that the use of robots for ultrasound-guided nerve blocks is associated with faster learning and a lower inter-subject variability than manual performance in a simulated setting (Morse et al. 2014).

Other Applications
Good clinical practice can be enhanced by the use of decision support systems (DSS) and telemedicine. Decision support systems are designed to provide the performer with updated clinical suggestions and options for treatment. They are precursors of robots, able to detect adverse events and enhance compliance with guidelines. It has been shown that DSS are effective in facilitating the achievement of haemodynamic (Sondergaard et al. 2012) and ventilation (Blum et al. 2013) set points, with a performance at least the same as the one of the anaesthesiologist. DSS improve the detection and the management of intraoperative hyper- and hypotension (Nair et al. 2014), critical events (respiratory and haemodynamic) during sedation (Zaouter et al. 2014) and epidural haematoma in patients under anticoagulant or antiplatelet therapy (Gupta 2014). Telemedicine is a form of delivery of healthcare using information and communication technologies when distance between the providers is significant (Chatrath et al. 2010). Many applications in anaesthesia are currently under development, ranging from pre- and intra- to postoperative applications, with promising results (Chatrath et al. 2010; Galvez et al. 2011). This is highly advantageous for some rural areas of the world where there may be a paucity of physicians and healthcare facilities (Chatrath et al. 2010), as well as an additional opportunity for training and learning (Galvez et al. 2011). The remote control of general anaesthesia has been successfully performed between two different countries (Canada and Italy) by using robots (McSleepy) (Hemmerling et al. 2013c). This pilot study in 20 patients undergoing thyroid surgery in Italy showed the feasibility of teleanaesthesia, with no additional risk of complications (Hemmerling et al. 2013c). Remote preoperative airway assessment between the same two countries has been demonstrated to be feasible as well (unpublished data).
Conclusions
Robots in anaesthesia are designed to eliminate the repetitive part of the workload. The objective is to safely and effectively deliver anaesthesia and have control of all biological variables involved in homeostasis, which is at the base of a good patient outcome. Robots can be helpful to exert this control continuously and simultaneously, with anaesthesiologists having the possibility to 'open the loop' when needed. The automatic management of general anaesthesia, sedation and manual tasks is not inferior to the conduct of anaesthesiologists, but can be even better. Decision support systems and teleanaesthesia can significantly improve the quality of care and the opportunity for training. Additional studies are needed to further test the safety of robots and to develop more refined systems of control and monitoring in order to integrate all components of the management of anaesthesia, augmenting their reliability and overcoming the possible limitations related to their use.
References:
Absalom A, Kenny G (2003) Closed‐loop control of propofol anaesthesia using bispectral index™: performance assessment in patients receiving computer‐controlled propofol and manually controlled remifentanil infusions for minor surgery. Br J Anaesth, 90(6): 737-41.PubMed ↗
Atchabahian A, Hemmerling TM (2014) Robotic anesthesia: how is it going to change our practice? Anesth Pain Med, 4(1): e16468. PubMed ↗
Banerjee S, Desilets D, Diehl DL et al. (2011) Computer-assisted personalized sedation. Gastrointest Endosc, 73(3): 423-7. PubMed ↗
Bickford RG (1950) Automatic electroencephalographic control of general anesthesia. EEG Clin Neurophysiol, 2: 93-6. Article ↗
Blum JM, Stentz MJ, Maile MD et al. (2013) Automated alerting and recommendations for the management of patients with preexisting hypoxia and potential acute lung injury. Anesthesiology, 119(2): 295-302. PubMed ↗
Burns KE, Lellouche F, Lessard MR et al. (2014) Automated weaning and spontaneous breathing trial systems versus non‐automated weaning strategies for discontinuation time in invasively ventilated postoperative adults. Cochrane Database Syst Rev, 2:CD008639. doi: 10.1002/14651858.CD008639.pub2. PubMed ↗
Cannesson M, Rinehart J (2014) Closed-loop systems and automation in the era of patients safety and perioperative medicine. J Clin Monit Comput, 28(1): 1-3. PubMed ↗
Chatrath V, Attri JP, Chatrath R (2010) Telemedicine and anaesthesia. Indian J Anaesth, 54(3): 199-204. PubMed ↗
Dumont GA, Ansermino JM (2013) Closed-loop control of anesthesia: a primer for anesthesiologists. Anesth Analg, 117(5): 1130-8. PMID: 23835456 PubMed ↗
Dumont G, Liu N, Petersen C et al. (2011) Closed-loop administration of propofol guided by the NeuroSense: clinical evaluation using robust proportional-integral-derivative design. American Society of Anesthesiologists Annual Meeting, 15-19 October, Chicago, Illinois, USA. [Abstract] [Accessed: 21 February 2014] Available from asaabstracts.com/strands/asaabstracts/abstract.htm;jsessionid=6A826E2C608C8C9A0C6EA01F56953852?year=2011&index=8&absnum=5659
Fang M, Tao Y, Wang Y (2014) An enriched simulation environment for evaluation of closed-loop anesthesia. J Clin Monit Comput, 28(1): 13-26. PubMed ↗
Galvez JA, Rehman MA (2011) Telemedicine in anesthesia: an update. Curr Opin Anaesthesiol, 24(4): 459-62. PubMed ↗
Gentilini A, Rossoni-Gerosa M, Frei CW et al. (2001) Modeling and closed-loop control of hypnosis by means of bispectral index (BIS) with isoflurane. IEEE Trans Biomed Eng, 48(8): 874-89. PubMed ↗
Goudra BG, Singh PM, Chandrasekhara V (2014) SEDASYS, airway, oxygenation, and ventilation: anticipating and managing the challenges. Dig Dis Sci, 59(5):920-7. PubMed ↗
Gupta RK (2012) Using an electronic clinical decision support system to reduce the risk of epidural hematoma. Am J Ther, 21(5):327-30. PubMed ↗
Hallenberger A, Poets CF, Horn W et al. (2014) Closed-loop automatic oxygen control (CLAC) in preterm infants: A randomized controlled trial. Pediatrics, 133(2): e379-85. PubMed ↗
Hemmerling TM, Charabati S, Zaouter C et al. (2010a) A randomized controlled trial demonstrates that a novel closed-loop propofol system performs better hypnosis control than manual administration. Can J Anaesth, 57: 725-35. PubMed ↗
Hemmerling T, Zaouter C, Tang L et al. (2010b) McSleepy-a novel completely automatic anesthesia delivery system: performance evaluation in comparison to manual control. Abstract 803213. Can J Anesth, 57(1 Suppl): S116. Article ↗
Hemmerling TM, Taddei R, Wehbe M et al. (2011a) Robotic anesthesia – a vision for the future of anesthesia. Transl Med UniSa, 1: 1-20. PubMed ↗
Hemmerling TM, Arbeid E, Tang L et al. (2011b) HSS - A novel hybrid system for conscious sedation. Anesth Analg, 113: 39.
Hemmerling TM, Wehbe M, Zaouter C et al. (2012a) The Kepler intubation system. Anesth Analg, 114(3): 590-4. PubMed ↗
Hemmerling TM, Taddei R, Wehbe M et al. (2012b) First robotic tracheal intubations in humans using the Kepler intubation system. Br J Anaesth, 108(6): 1011-6. PubMed ↗
Hemmerling TM, Terrasini N (2012) Robotic anesthesia: not the realm of science fiction any more. Curr Opin Anesthesiol, 25(6): 736-42. PubMed ↗
Hemmerling TM, Arbeid E, Wehbe M et al. (2013a) Evaluation of a novel closed-loop total intravenous anaesthesia drug delivery system: a randomized controlled trial. Br J Anaesth,110(6): 1031-9. PubMed ↗
Hemmerling TM, Taddei R, Wehbe M et al. (2013b) Technical communication: First robotic ultrasound-guided nerve blocks in humans using the Magellan system. Anesth Analg, 116(2): 491-4. PubMed ↗
Hemmerling TM, Arbeid E, Wehbe M et al. (2013c) Transcontinental anaesthesia: a pilot study. Br J Anaesth, 110(5): 758-63. PubMed ↗
Le Guen M, Grassin-Delyle S, Cornet C et al. (2014) Comparison of the potency of different propofol formulations: a randomized, double-blind trial using closed-loop administration. Anesthesiology, 120(2): 355-64. PubMed ↗
Liberman MY, Ching S, Chemali J et al. (2013) A closed-loop anesthetic delivery system for real-time control of burst suppression. J Neural Eng, 10(4): 046004. PubMed ↗
Liu N, Chazot T, Hamada S et al. (2011) Closed-loop coadministration of propofol and remifentanil guided by bispectral index: a randomized multicenter study. Anesth Analg, 112(3): 546-57. PubMed ↗
Liu N, Le Guen M, Benabbes-Lambert F et al. (2012) Feasibility of closed-loop titration of propofol and remifentanil guided by the spectral M-Entropy monitor. Anesthesiology, 116(2): 286-95. PubMed ↗
Luria I, Lampotang S, Schwab W et al. (2013) Automated, real-time fresh gas flow recommendations alter isoflurane consumption during the maintenance phase of anesthesia in a simulator-based study. Anesth Analg, 117(5): 1139-47. PubMed ↗
Morse J, Wehbe M, Taddei R et al. (2013) Magellan: Technical description of a new system for robot-assisted nerve blocks. J Comput, 8: 1401-5.
Morse J, Terrasini N, Wehbe M et al. (2014) Comparison of success rates, learning curves, and inter-subject performance variability of robot-assisted and manual ultrasound-guided nerve block needle guidance in simulation. Br J Anaesth, 112(6):1092-7. PubMed ↗
Nair BG, Horibe M, Newman SF et al. (2014) Anesthesia information management system-based near real-time decision support to manage intraoperative hypotension and hypertension. Anesth Analg, 118(1): 206-14. PubMed ↗
Puri GD, Kumar B, Aveek J (2007) Closed-loop anaesthesia delivery system (CLADS) using bispectral index: a performance assessment study. Anaesth Intensive Care, 35(3): 357-62. PubMed ↗
Puri GD, Jayant A, Tsering M et al. (2012) Closed loop anaesthesia at high altitude (3505 m above sea level): performance characteristics of an indigenously developed closed loop anaesthesia delivery system. Indian J Anaesth, 56(3): 238-42. PubMed ↗
Rinehart J, Chung E, Canales C et al. (2012) Intraoperative stroke volume optimization using stroke volume, arterial pressure, and heart rate: closed-loop (learning intravenous resuscitator) versus anesthesiologists. J Cardiothorac Vasc Anesth, 26(5): 933-9. PubMed ↗
Rinehart J, Lee C, Cannesson M et al. (2013a) Closed-loop fluid resuscitation: robustness against weight and cardiac contractility variations. Anesth Analg, 117(5): 1110-8. PubMed ↗
Rinehart J, Lee C, Canales C et al. (2013b) Closed-loop fluid administration compared to anesthesiologist management for hemodynamic optimization and resuscitation during surgery: an in vivo study. Anesth Analg, 117(5): 1119-29. PubMed ↗
Singaravelu S, Barclay P (2013) Automated control of end-tidal inhalation anaesthetic concentration using the GE Aisys Carestation™. Br J Anaesth, 110(4): 561-6.PubMed ↗
Smith AF, Greaves JD (2010) Beyond competence: defining and promoting excellence in anaesthesia. Anaesthesia, 65(2): 184-91. PubMed ↗
Sng B, Tan H, Sia A (2014) Closed‐loop double‐vasopressor automated system
vs manual bolus vasopressor to treat hypotension during spinal anaesthesia for
caesarean section: a randomised controlled trial. Anaesthesia, 69: 37-45. PubMed ↗
Sondergaard S, Wall P, Cocks K et al. (2012) High concordance between expert anaesthetists' actions and advice of decision support system in achieving oxygen delivery targets in high-risk surgery patients. Br J Anaesth, 108(6): 966-72. PubMed ↗
Tighe PJ, Badiyan SJ, Luria I et al. (2010a) Robot-assisted airway support: a simulated case. Anesth Analg, 111(4): 929-31.PubMed ↗
Tighe PJ, Badiyan SJ, Luria I et al. (2010b) Technical communication: robot-assisted regional anesthesia: a simulated demonstration. Anesth Analg, 111(4): 813-6. PubMed ↗
Wang Y, Xie H, Jiang X et al. (2014) Intelligent closed-loop insulin delivery systems for ICU patients. IEEE J Biomed Heath Inform, 18(1): 290-9.PubMed ↗
Wehbe M, Arbeid E, Cyr S et al. (2014) A technical description of a novel pharmacological anesthesia robot. J Clin Monit Comput, 28: 27-34. PubMed ↗
Webhe M, Morse J, Taddei R et al. (2012) Automatic ultrasound nerve detection. Society for Technology in Anesthesia Annual Meeting. [Abstract] [Accessed: 24 February 2014 Available from stahq.org/files/4613/2743/1056/Abstract_43.pdf
West N, Dumont GA, van Heusden K et al. (2013) Robust closed‐loop control of induction and maintenance of propofol anesthesia in children. Paediatric Anaesth, 23 (8): 712-9. PubMed ↗
Zaouter C, Taddei R, Wehbe M et al (2016) A novel system for automated propofol sedation: hybrid sedation system (HSS). J Clin Monit Comput, Mar 12. [Epub ahead of print] PubMed ↗
Zaouter C, Wehbe M, Cyr S et al. (2014) Use of a decision support system improves the management of hemodynamic and respiratory events in orthopedic patients under propofol sedation and spinal analgesia: a randomized trial. J Clin Monit Comput, 28(1): 41-7. PubMed ↗

