HealthManagement, Volume 22 - Issue 4, 2022
 PRINT OPTIMISED
PRINT OPTIMISED
Key Points
- New technological approaches such as Brain-Computer Interface (BCIs) solutions may address current unmet clinical needs and improve patients’ quality of life.
- Most innovations in healthcare are incremental and there is a gap between their conceptualisation and their adoption into healthcare systems.
- A collaborative environment from all the stages of research and development of BCIs in healthcare contexts is needed to improve the chance of making these devices available for every patient in need.
- When developing BCIs engineers need to prioritise security, reliability and usability for easier adoption in healthcare.
- Healthcare professionals should be patient advocates, demanding BCIs to be patient-centred, have a tailored approach to each case and never forget ethics.
- Management priorities should lie in integration of this technology into healthcare pathways, foster collaboration both between multidisciplinary areas of science but also engaging and collaborating with other stakeholders and have a continuous improvement plan
- Managers play a pivotal role in the successful adoption of BCIs as they may act as awareness raising agents and facilitators of multidisciplinary collaboration between areas of science, multiple stakeholders and patients, bringing them to the centre of value-generating future care.
Introduction
Patients can be directly linked to data via Brain-Computer Interfaces (BCIs). Through them people are ultimately linked to computers via data, with data analytics and artificial intelligence (AI) playing a big role in this linkage.
Illness or injury that results in damage to the brain and its functions can lead to serious dysfunction and disability. Although new functional connections may be formed, the brain has a limited capacity to repair damaged tissue (Baldwin et al. 2013).
High global incidence of neurological and mental health disorders generates considerable economic burden, not only through direct healthcare costs but also in lost productivity (Baldwin et al. 2013; Simeral et al. 2021). There is a paucity of effective treatments for some of these disorders which means the accumulation of unmet health and healthcare needs.
Innovative approaches that counteract the varied impacts of these diseases on social, economic and everyday life of patients and their families are needed (Camargo-Vargas et al. 2021). Novel neurotechnologies offer potential routes to meet some of these needs, but pathways to mainstream innovative and effective treatments are still a challenge.
Hospital and healthcare managers should be seen as innovation agents, particularly when technologies that are promising and could open windows of hope to certain groups of patients are maturing but need some help to become mainstream. It is important for health management to know about cutting edge neurotechnology as this is likely to be one of the future differentiating factors in large healthcare organisations and not just some academic health centres.
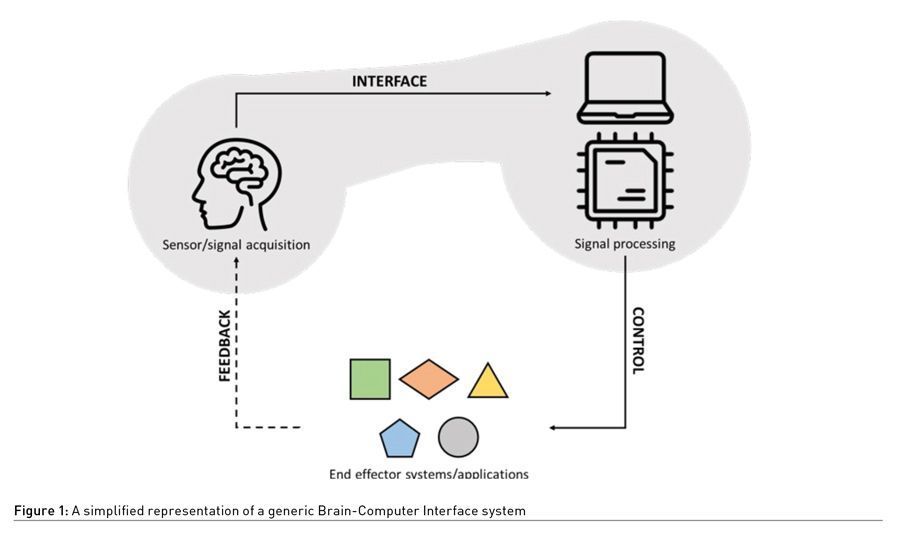
Brain-Computer Interface (BCI) (Figure 1) is an emerging neurotechnology, that is defined as “a communication system in which messages or commands that an individual sends to the external world do not pass through the brain’s normal output pathways of peripheral nerves and muscles”, providing “an alternative method for acting on the world” (McFarland and Wolpaw 2002).
BCIs for Rehabilitation and Restoration
BCIs’ potential applications to clinical conditions include rehabilitation and partial restoration of lost neurological function (Bockbrader et al. 2018). Most of these potential applications correspond to medical conditions that have no satisfying current therapeutic options.
BCIs are used to replace lost neurologic function by restoring patients’ ability to interact with and control various environments and activities. For example, mobility devices or neuroprosthetic limbs and orthoses (Bockbrader et al. 2018). They can also be used with rehabilitative therapies to help restore normal central nervous system function by synchronising brain activity that corresponds to movement intent with actual movements and sensations generated by end-effector devices, inducing brain plasticity (Bockbrader et al. 2018).
BCIs have been used as investigational assistive devices for individuals with chronic paralysis from multiple causes, including cervical spinal cord injury (SCI), spinocerebellar degeneration, amyotrophic lateral sclerosis (ALS) and brainstem stroke (Bockbrader et al. 2018).
From a care perspective, BCIs may assist users to communicate, control prostheses or wheelchairs, and support rehabilitation (Baldwin et al. 2013); therefore they might be significant to help managing, and in the future even treating, these conditions (Camargo-Vargas et al. 2021).
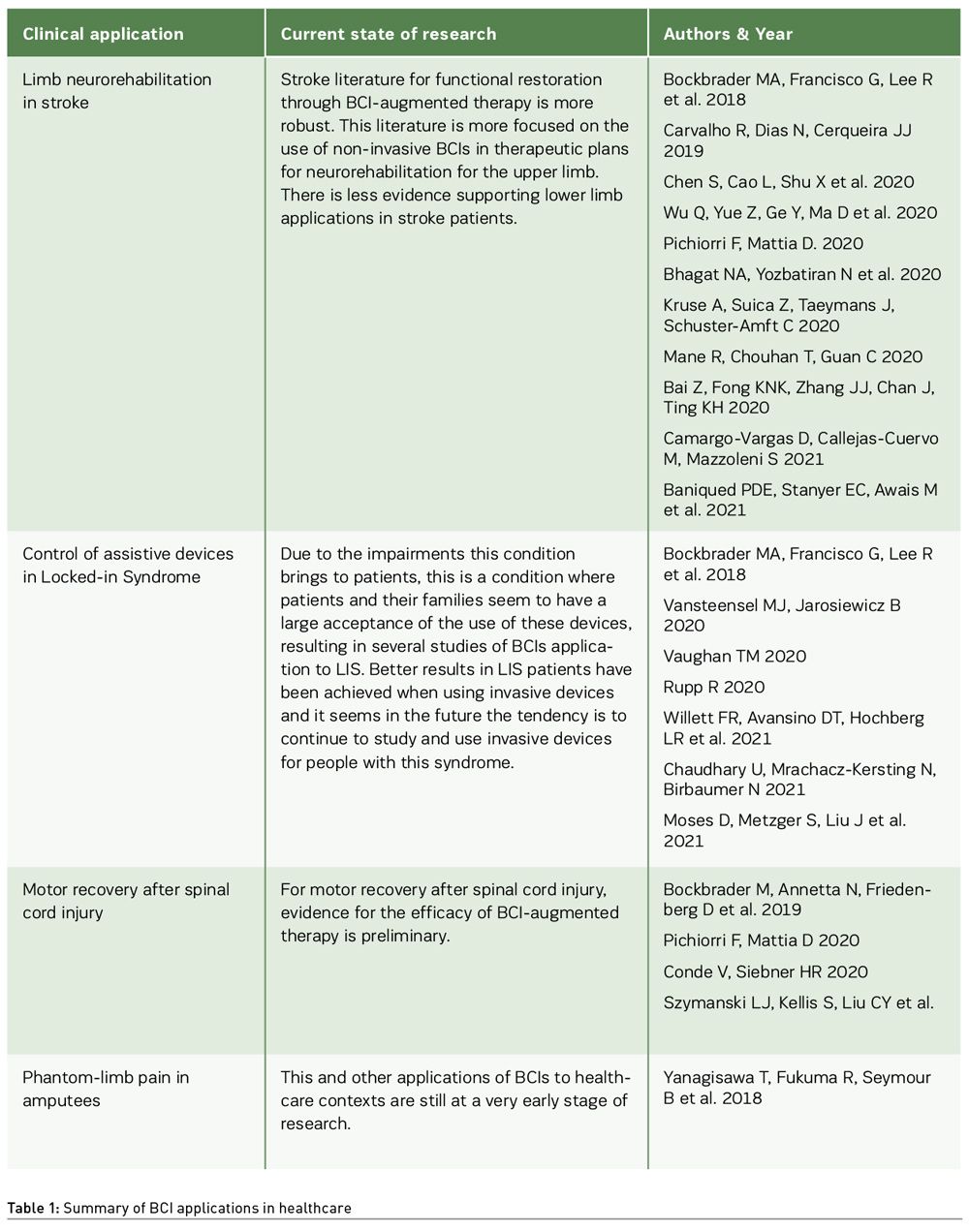
Table 1 provides a broad view of the potential clinical applications of BCIs. While this this is not an extensive description of all potential clinical applications or studies of BCIs in
healthcare, it serves as a set of illustrative examples.
While BCIs adoption seems to be lagging in clinical contexts, direct-to-consumer BCIs seem to be in a new phase of hype as an extended reality technology (Hall and Baier-Lentz 2022). These direct-to-consumer devices can be used by citizens as wellness devices. Some authors claim they can even impact users’ health and could be used to improve physical, mental, and social well-being (Thomas et al. 2013; Faller et al. 2019; Coates and Wexler 2020).
The spread of direct-to-consumer BCIs raises even more concerns about confidentiality and security of personal brain data. Cybersecurity risks are known and are real in both healthcare and in general contexts. Data security, data misuse and privacy breaches are a real risk, so it is essential to establish safeguards at the system level to minimise these device risks, and preferably an institutional rather than an individual ad-hoc approach should be stimulated by policymakers and health managers to counter these risks by assuming, accepting and embracing these technologies.
Widespread Clinical Adoption of BCIs
Although BCIs have demonstrated potential use in clinical settings, including patients home, the use of these devices is still confined to research contexts (Baldin et al. 2013; Bockbrader et al. 2018; Hall and Baier-Lentz 2022).
Currently, BCIs are recognised as a technology with potential to influence the future of healthcare and medicine and have been gaining spotlight, raising more investment to research (Future Today Institute 2022). Nonetheless, large and mainstream clinical adoption is lagging as several challenges need to be addressed.
In the healthcare sector, innovations like BCIs have the potential to improve some patients’ quality of life (QoL), but they also offer a challenge to existing providers and systems to its adoption. Most innovations in healthcare are incremental and disruptive innovations are rare (Flessa and Huebner 2021). The more disruptive a new technology is, the bigger the gap between its conceptualisation and its adoption into healthcare systems (Vomero and Schiavone 2021) and these technologies often face hurdles in their commercialisation that impact their clinical adoption (Pulliam et al. 2022).
Neurotechnology is a complex field and calls for a more comprehensive and multidisciplinary approach for its development and adoption (Stieglitz 2021). Not only is there a need to stimulate interdisciplinary work between Health and Engineering, Social and Behavioural Sciences but to also know how to engage patients and caregivers well throughout the Research and Development (R&D) process. The discussion of a clear path, which considers guidelines and agreed standards, towards translation of BCIs to clinical practice, may facilitate adoption by health systems when these devices reach the appropriate maturity level for large-scale adoption.
To mature neurotechnology in the context of the health heavy regulated sector takes time, investment and stamina from multiple stakeholders. The need for integration of different areas of knowledge and to improve technological literacy is not only beneficial for these technologies and innovations but can contribute with new perspectives and approaches which can bring more innovation and other improvements to health systems. Healthcare is said to be conservative and slow in adopting changes, requiring robust evidence for safety and clinical benefits. This is likely to be the case for the widespread adoption of BCIs.
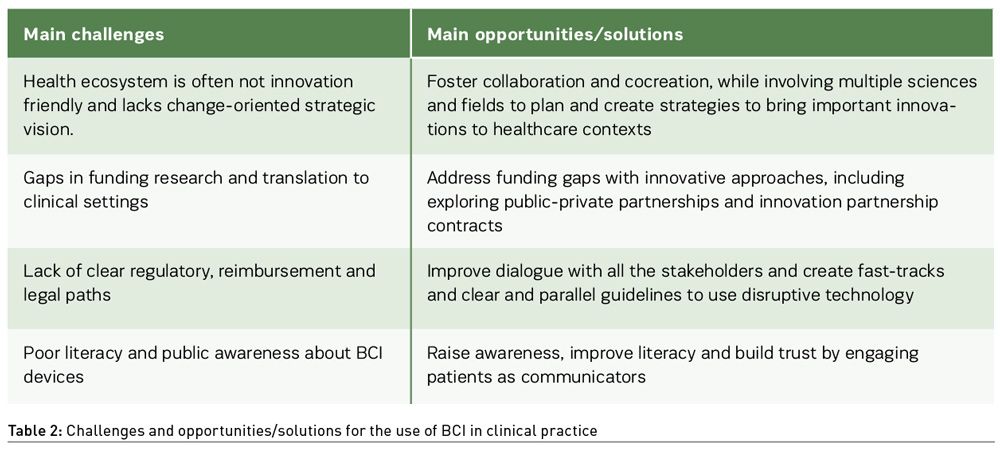
Table 2 briefly resumes some challenges and opportunities to consider while introducing disruptive technologies, like BCIs, into healthcare contexts.
When thinking about the translation of BCIs into widespread adoption in clinical settings it is important to take into consideration the continuous investment to fund research and improvement of the device, as well as understand how healthcare professionals and patients will react differently to the innovation in the specific context of implementation.
Multidisciplinary efforts, engaging patients and healthcare professionals more and a framework embodying clinically relevant outcomes for patients are needed for progress to be made. Also, a clear Health Technology Assessment (HTAs) methodology for BCI technology would be useful for a better classification and characterisation of the different BCIs’ clinical applications that have better evidence of being closer to a translation into healthcare practices. This evaluation would include clear information and indications regarding the condition to be addressed as well as potential risks and expected benefits.
This may be a small step but will always be a step towards the creation of clinical guidelines and future integration of this neurotechnology in the health systems leading to a wide clinical adoption.
A range of opportunities where BCIs may provide significant health, societal, and economic value speak to the long-term potential of the field. Many of these applications are still in the pre-clinical, experimental, or theoretical stage.
Now is the time to be aware of these future trends and start to prepare for better adoption of enabling BCI technologies in healthcare. It is also a time to facilitate the generation of additional evidence about clinical outcomes to boost future of health policy in this field. Finally, it is time to tackle barriers to widespread clinical adoption of BCIs and catalyse opportunities across the healthcare ecosystem while stimulating a culture of innovation that accelerates the deployment of BCI-based solutions for use in clinical settings.
It is also important to show benefit for potential users by agreeing on health outcome definitions and measurement in light of these very complex therapeutic interventions. This comprehension will also be enhanced by an agreement on standardised approaches to presenting information and on criteria that are linked to context and recognise that they are overlapping and could require emphasis depending on the decision-making actor and perspective.
A simple 3x3 model for development and translation of BCIs in healthcare (Figure 2) is proposed, assuming three priorities for three distinct scientific areas that need to work in collaboration and coordination: Engineering, Medicine and Management. Engineering should prioritise security, reliability and usability of BCIs when developing them. Medicine critical aspects include patient-centredness, a tailored approach to each case and the management of risks and ensuring clinical benefits while not forgetting ethics. For Management the priorities are integration of this technology into healthcare pathways, foster collaboration both between multidisciplinary areas of science but also engage and collaborate with other stakeholders and have a continuous improvement plan.
![]()
Glimpse into the Future and Brain Data
BCIs seem to be at a turning point. In recent years research has been raising the bar and its potential for clinical use seem stronger. A new phase of hype and even adoption of BCIs as a direct-to-consumer device may help BCIs stepping out of the lab-bench and successfully achieve widespread clinical adoption. Promising trials and positive outcomes with relevance for the patients are laying the foundation.
When (and if) BCIs reach clinical practice (regulated as “advanced” medical devices, almost always involving some AI technologies, and hence under AI regulation scope as well) and if clinicians will readily accept these changes and prescribe the devices remains to be seen. The integration of medical doctors in the teams developing BCIs may bring some confidence to other clinicians, but other initiatives to raise awareness and knowledge of these devices as well as their integration in clinical guidelines may push further its adoption.
This adoption will not depend only on clinicians. Engaging with a wide variety of stakeholders, understanding their perspectives and winning confidence and support will help to guide progress for the use of BCIs in healthcare contexts. To understand particularities of the health system itself and how it can adapt towards patients’ needs, to guarantee it is the best solution possible and tailored to the patient needs and demands, meeting their expectations, but also to ensure equity of access for the those that may need them, would be crucial to the successful implementation of BCIs as a therapeutic tool.
A widespread clinical adoption of neurotechnologies like BCIs faces several ethical and legal concerns (Ienca 2021). One of the most increasing concerns represent the availability of brain data acquired by BCIs, which combined with the application of AI to brain data analysis, poses a challenge for ethics and governance (Ienca et al. 2021).
On one hand, an increasing volume and variety of brain data may be crucial for research and to advance the scientific understanding of the human brain and provide preventive, diagnostic and therapeutic solutions for patients with neurological or psychiatric disorders. On the other hand, brain data is still data and part of a wider digital ecosystem, being therefore subject to the same risks and vulnerabilities as other digital data.
Brain data obtained by BCIs will have the power to support evidence-based decisions, but this data still needs to be shared so it may contribute to new discoveries in the research of brain mechanisms. We argue this data should be shared, but how to do it is still unclear. Use of biodata banks, where patients are able to consent to their brain data usage for research purposes may be one way. Patients might be more willing to share data if its use is for their benefit or benefit of future patients. However, it is important to acknowledge that this willingness may shift if there is data misuse by the organisations.
An informed consent from the patients for the use and availability of their own brain data, while respecting privacy, are central parts on building a sustainable future for brain (health) data.
It is also important to start this discussion in the dawn of the European Health Data Space and how this brain data should be integrated not only in the personal space of the patient but also be digitally available for organisations and professionals responsible for the care and for other researchers. The amounts of data acquired and generated make it obvious that its analysis will require automation. AI tools will be responsible for not only analysing and categorising data but will also play a role on future developments by, for example, understanding hidden patterns in this data and extracting meaningful markers from the data obtained from the brain.
Implications for Hospitals and Healthcare Managers
In healthcare, successful innovations bring clear benefits when compared to what is currently done, and often possess two key qualities: they are both usable and desirable (Kelly and Young 2017).
New clinical technologies have the potential to bring important benefits to healthcare; however, achieving an optimal spread of new clinical technologies into healthcare has proved to be far from straightforward (Llewellyn et al. 2014).
Successful implementation of technology depends on negotiating the changes this requires to staff activities and adapting implementation to the wider organisational and social context (Llewellyn et al. 2014).
Hospital and healthcare managers may have a pivotal role to play in the successful adoption of BCIs into widespread clinical contexts. As referred before, their role as facilitators of collaboration between multidisciplinary areas of science, collaborate with other stakeholders and define a continuous improvement plan would be part of a successful adoption. On the other hand, they may also act as facilitators of the awareness in communities where they are integrated into, contributing to bringing patients to the table to establish a plan that brings value and addresses their needs.
Understanding data as foundation for increased quality and accelerated improvement and safety, leading to better and more suitable to the users’ devices, should make healthcare managers have a comprehensive approach to data governance. Data-driven interventions while ensuring highest data protection standards and a secure data space providing access to quality-checked, anonymised health data for medical research and development will contribute to better patients’ life and to raise trust in AI and its potential in the field of neurotechnology. To have a patient-centred approach to brain health data, should premise patient participation in the decisions regarding their data, in a shared responsibility process.
Besides this, hospital and healthcare managers must also think ahead in the future. The current trend on domiciliary and telehealth care may change the current picture of health facilities. If these trends grow in the future, hospitals may redefine part of their role and act, for example, as a hub to integrate healthcare professionals, other professionals acting in health like engineers, academia, industry and all the relevant stakeholders. On this note, they have a key role in starting a cycle of valuable innovation adoption with consequent gains for the patients and for the healthcare system.
Co-creation and collaborative environments may shift the current landscape towards a more innovation friendly ecosystem which would comprise more value for the patient, but also more value for the society and for innovative businesses with valuable propositions. Science and technology alone will not change healthcare or the world. Instead, a strategic vision and leadership are needed in order to surpass barriers, innovate and successfully implement new strategies to past, present and future problems.
Conflict of Interest
None. 
References:
Bai Z, Fong KNK, Zhang JJ et al. (2020) Immediate and long-term effects of BCI-based rehabilitation of the upper extremity after stroke: a systematic review and meta-analysis. J NeuroEngineeringRehabil. 17(1):1–20.
Baniqued PDE, Stanyer EC, Awais M et al. (2021) Brain–computer interface robotics for hand rehabilitation after stroke: a systematic review. J NeuroEngineeringRehabil. 18(1):1–25.
Bhagat NA, Yozbatiran N, Sullivan JL et al. (2020) Neural activity modulations and motor recovery following brain-exoskeleton interface mediated stroke rehabilitation. NeuroImage Clin. 1;28:102502.
BaldwinT, Fitzgerald M, Kitzinger J et al. (2013) Novel neurotechnologies: intervening in the brain. Nuffield Council on Bioethics. 298.
Bockbrader MA, Francisco G, Lee R et al. (2018) Brain Computer Interfaces in Rehabilitation Medicine. PM&R. 10(9):S233–43.
Camargo-Vargas D, Callejas-Cuervo M, Mazzoleni S (2021) Brain-Computer Interfaces Systems for Upper and Lower Limb Rehabilitation: A Systematic Review. Sensors. 21(13):4312.
Carvalho R, Dias N, Cerqueira JJ (2019) Brain-machine interface of upper limb recovery in stroke patients rehabilitation: A systematic review. Physiother Res Int. 24(2).
Chaudhary U, Mrachacz-Kersting N, Birbaumer N (2021) Neuropsychological and neurophysiological aspects of brain-computer-interface (BCI) control in paralysis. J Physiol. 599(9):2351–9.
Chen S, Cao L, Shu X et al. (2020) Longitudinal Electroencephalography Analysis in Subacute Stroke Patients During Intervention of Brain–Computer Interface With Exoskeleton Feedback. Front Neurosci. 14;0:809.
Coates MI, Wexler A (2020) Peering into the mind? The ethics of consumer neuromonitoring devices,” in Ethical Dimensions of Commercial and DIY Neurotechnologies, eds I. Bard and E. Hildt. Cambridge, MA: Elsevier, Academic Press. 1–22.
Conde V, Siebner HR (2020) Brain damage by trauma. Handb Clin Neurol. 168:39–49.
Faller J, Cummings J, Saproo S, Sajda P (2019) Regulation of arousal via online neurofeedback improves human performance in a demanding sensory-motor task. PNAS.
Flessa S, Huebner C (2021) Innovations in health care - a conceptual framework. Int J Environ Res Public Health. 18(19).
Future Today Institute. Health & Medicine. Tech Trends Report. (2022) Available from https://eur-lex.europa.eu/legal-content/PT/TXT/PDF/?uri=CELEX:32016R0679&from=PT%0Ahttp://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=CELEX:52012PC0011:pt:NOT.
Hall SB, Baier-Lentz M (2022) The future of the metaverse will be shaped by these 3 technologies | World Economic Forum. Available from https://www.weforum.org/agenda/2022/02/future-of-the-metaverse-vr-ar-and-brain-computer/
Ienca M (2021) Common Human Rights Challenges Raised By Different Applications of Neurotechnologies in the Biomedical Field.
Ienca M, Fins JJ, Jox RJ et al. (2021)Towards a Governance Framework for Brain Data. ArXiv preprint 2109.11960.
Kelly CJ, Young AJ (2017) Promoting innovation in healthcare. FuturHealthc J. 4(2):121–5.
Kruse A, Suica Z, Taeymans J, Schuster-Amft C (2020) Effect of brain-computer interface training based on non-invasive electroencephalography using motor imagery on functional recovery after stroke - a systematic review and meta-analysis. BMC Neurol. 20(1):1–14.
Llewellyn S, Procter R, Harvey G et al. (2014). Facilitating technology adoption in the NHS: negotiating the organisational and policy context – a qualitative study. Heal ServDeliv Res. 2(23):1–132.
Mane R, Chouhan T, Guan C (2020) BCI for stroke rehabilitation: motor and beyond. J Neural Eng. 17(4):041001.
McFarland DJ, Wolpaw JR (2002) Brain-computer interfaces for communication and control. Commun ACM. 54(5):60–6.
Moses DA, Metzger SL, Liu JR et al. (2021) Neuroprosthesis for Decoding Speech in a Paralyzed Person with Anarthria. NEJM. 385(3):217–27.
Neuper C, Müller GR, Kübler A et al. (2003) Clinical application of an EEG-based brain–computer interface: a case study in a patient with severe motor impairment. Clin Neurophysiol. 114(3):399–409.
Pichiorri F, Mattia D (2020) Brain-computer interfaces in neurologic rehabilitation practice. Handb Clin Neurol. 168:101–16.
Pulliam CL, Stanslaski SR, Denison TJ (2020) Industrial perspectives on brain-computer interface technology. First Edition. Handbook of Clinical Neurology. Elsevier BV. 168:341–352.
Rupp R (2020) Spinal cordlesions. Handb Clin Neurol. 168:51–65.
Simeral JD, Hosman T, Saab J et al. (2021) Home use of a percutaneous wireless intracortical brain-computer interface by individuals with tetraplegia. IEEE Trans Biomed Eng. 68(7):2313–25.
Stieglitz T (2021) Why Neurotechnologies? About the Purposes, Opportunities and Limitations of Neurotechnologies in Clinical Applications. Neuroethics. 14(1):5–16.
Szymanski LJ, Kellis S, Liu CY et al. (2021) Neuropathological effects of chronically implanted, intracortical microelectrodes in a tetraplegic patient. J Neural Eng. 18(4):0460b9.
Thomas KP, Vinod AP, Guan C (2013) Design of an online EEG based neurofeedback game for enhancing attention and memory, 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). 433-436.
Vansteensel MJ, Jarosiewicz B (2020) Brain-computer interfaces for communication. Handb Clin Neurol. 168:67–85.
Vaughan TM (2020) Brain-computer interfaces for people with amyotrophic lateral sclerosis. Handb Clin Neurol. 168:33–8.
Vomero M, Schiavone G (2021) Biomedical microtechnologies beyond scholarly impact. Micromachines. 12(12):1–11.
Yanagisawa T, Fukuma R, Seymour B et al. (2018) MEG–BMI to Control Phantom Limb Pain. Neurol Med Chir (Tokyo). 58(8):327–33.
Willett FR, Avansino DT, Hochberg LR et al. (2021) High-performance brain-to-text communication via handwriting. Nature. 593(7858):249–54.
Wu Q, Yue Z, Ge Y et al. (2020) Brain Functional Networks Study of Subacute Stroke Patients With Upper Limb Dysfunction After Comprehensive Rehabilitation Including BCI Training. Front Neurol. 0:1419.

