HealthManagement, Volume 15 - Issue 3, 2015
The future of primary care in the global health approach
Background and Trends
Healthcare services have been under great pressure during recent years, especially when the economic and financial crisis put a remarkable emphasis on sustainability.
It is generally accepted that developed countries’ economies are not going to grow until infinity and the capacity of the emergent economies to lead the world economy is not guaranteed. From another point of view, it seems more accepted that the right to access healthcare services should overcome cultural and economic circumstances and is a “fundamental right”.
In this context there appears the concept of “global health”, a translation of the concept of globalisation to the healthcare sector. “Our Health is Global Health” stated Alan R. Weil, Editor-in- Chief of Health Affairs on September 2014 under the concept of “Advancing Global Health Policy”.
A framework of global continuous learning has been established thanks to the improvement in access to relevant information and the ease of networking.
Convergence of Healthcare System Models
My point is that with the actual situation, and thanks to the probability of more velocity in the adoption of good practice worldwide, a global model of healthcare services is going to emerge. That means that, in the end, converging organisational financing and even coverage models of the worldwide healthcare systems will be developed. Of course, it will take some time due to cultural, political and economic differences among countries. I am not an expert on the theory of evolution of the species, of organisations or companies, but it seems clear that the trend is to converge, to benchmark and to take the best lessons home.
Let me share with you a conceptual thought: we agree on applying the concept of evidence in clinical practice known under the acronym EBM (evidence-based medicine). It was very successful some years ago and has been reinforced during recent years thanks to the advances in research methodologies and the possibility of discussing the results worldwide. This means that, if a procedure is based on evidence, it should be practised worldwide in the exact same way. We are not going to accept bad results due to a non evidence-based practice (of course here the role of the patient is clear).
Around any procedure, there is the concept of process, which needs an organisational context (not only) to be practised. I am going to summarise briefly because this is not the objective of this article: if we need to practise EBM, the organisation of the healthcare system should be based on the most cost-effective model which, in the end, is going to be very similar worldwide. If we agree on these concepts and, returning to the topic of this article, we should accept that there is a better model for efficiency of healthcare systems. It is generally accepted that the model should revolve around primary care with the team model. At this level, I think we can see the convergence. The team model, born under the Beveridge model (National Health Care Systems), is, among others, present in the primary care centres of the Scandinavian countries, Spain and the UK.
We can also see some changes in this direction in France (Maisons de santé), the Netherlands and Germany, which, however, follows the Bismarck model (Social Security Systems).
Finally, we can observe the powerful movement of the Medical Home in the US developed under the Affordable Care Act (2010) through the Accountable Care Organisations (ACO) model and based on the successes of Kaiser Permanente, Veterans Health Administration and Health Plans. This movement also changes the payment model from a fee-for-service to a payment for results and value. Bundled payments are moving in the same direction.
Primary Care (PC)
Let’s comment briefly on some aspects of PC which should be taken into consideration:
Generally speaking, it is most prestigious for a doctor to work as a specialist consultant in a hospital than in PC (it also means, in most cases, much better remuneration);
There is a lack of experience in working on processes at the PC level;
The role of nursing in PC is increasing (nurse specialists, nurse practitioners or advanced practice nursing), but we are only at the beginning of these experiences. Additionally, they are not developed globally and, in most cases, not well understood by doctors or healthcare managers;
One of the outcomes of this situation is that the relationships among PC, hospitals, public health and social services is poor. This lack of coordination goes against the main objective of PC, which is to work around the patient in all the aspects of their pathology(ies) from prevention, screening, diagnosis, treatment and follow-up and, if needed, end-of-life care;
The conceptual and, in some cases, ideological discussion around models and roles on “classic” PC probably has reached a point of no more progress.
The Computerisation of PC
In most countries, the level of computerisation in PC is lower than at the hospital level. Most facilities are not interoperable and, even in countries such as Spain where the level is high, the interoperability with hospitals or other levels or services (social care) is weak and the ability to share information between regions or with other European countries is not resolved (in spite of expensive and lengthy EU projects).
In any case, the computerisation of PC has allowed, as a first step, the organisation of clinical information, in most of the cases problem-oriented, which facilitated the exchange of information among PC professionals: physicians, nurses and in, some cases, hospital specialists.
Another problem has to be pointed out: the reliability and the relevance of the information. Indeed, hospitals have a Minimum Data Set (MDS) which, with the help of medical documentarists or similar professionals, has helped to structure and give reliability to the information shared. This is not the case with PC.
Moreover, the information that is relevant for one specialty (core of knowledge) is not relevant for another specialty and this gap is deeper between PC and specialists.
On the other hand, big advances have been made, with the computerisation of drug prescription and especially with the introduction of e-prescriptions. The quality of prescriptions has improved and the introduction of basic decision support system (DSS) has helped to identify problems (interactions and adverse reactions for example).
The introduction of Pay-for- Performance systems (P4P), based on registered information, has helped to control the cost and quality of prescriptions and the ordered referrals and exams. All these improvements have permitted us to reward or penalise good or poor practice.
Now, we are dealing with the introduction of information systems to help the development of integrated care so as to reach the coordination between healthcare providers and even social care providers. It is not easy because we should apply the concept of processes and reengineering to them to be successful which is going to take time. (This is not new; the Integrated Delivery Networks already emphasised this point about 30 years ago).
Big Data and Cognitive Computing
Now, once again, technology is making impressive advances; concept s like Big data, machine learning and cognitive computing (most of them an evolution of former concepts) are in the healthcare sector. In the field of oncology, the IBM Watson experience at the Cleveland and Mayo Clinics is giving excellent results. Some approaches have been implemented for medical homes, most of them acting as tools for decision support systems (DSS) in primary care. This topic is going to evolve depending on quality of data, level of integration and evolution of the process approach.
Triple Aim and Population Health Management
To advance in the globally accepted “Triple Aim approach” of the Institute for Healthcare Improvement (IHI) of Boston (better care, better patient experience and lower or at least controlled cost), we have to employ technology.
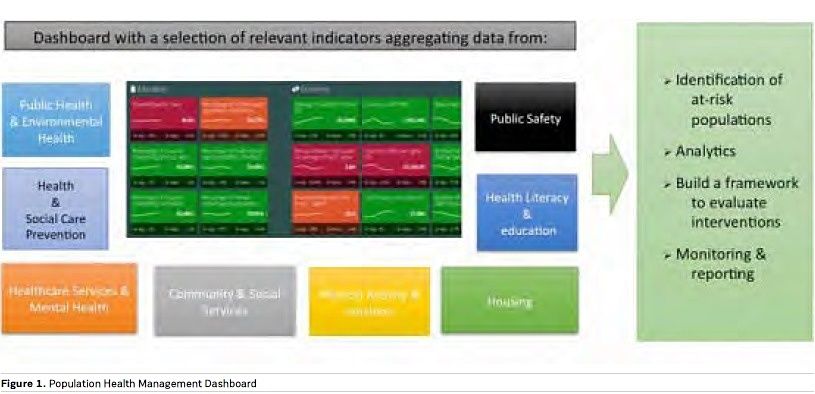
We also need a framework and the Population Health Management (PHM) approach seems to be the correct one. PHM strongly emerged recently thanks to the vision - among others - of the Dean Emeritus Stephen Shortell of the Berkeley School of Public Health. The King’s Fund has placed PHM only after the step of integrated care and some interesting experiences are arising in the US and the Netherlands. Only 25% of the concept is attributed to organisation of healthcare and healthcare services, the remaining percentage being attributed to other factors.
If we want to be preventive, predictive and proactive we should take decisions based on more data than that coming from the healthcare system (see Figure 1). The first step is to create a dashboard with integrated indicators coming from public health, social services, environmental health, housing and education. All of this is linked to concepts like smart cities. Owing to this, we are going to personalise interventions, beginning with the stratification of risk and, afterwards, monitoring and reporting the results.
The “Post-Industrialisation” Era of Healthcare: Vision of the Future
My main point is that to emphasise the vision of the future of healthcare systems, we should begin to work on the evolution of PC towards the PHM approach. As an example, this post-industrialisation era of healthcare opens the way to the computerisation of the patient healthcare journey around illness. With actual k nowledge, we can envision the future with a healthcare system centred on the patient, who is going to interact with “the systems” and will be assisted by more skilled nurses, fewer P C doc tors, ot her professionals from different sectors depending on the patient/citizen’s needs an d input from t he specialist, only when necessary.
Of course, evolution towards this mod e l won’t be immediate and some aspects have to be taken into consideration. The most important may be the discussion about the needs of doctors in t his future scenario. Dan Hoch, Director of Digital Initiatives Benson-Henry Institute, Massachuset ts General Hospital, stated in his blog on e-patients.net under the title Too Many Doctors?: “Much of what I do as a physician could be better d o ne by either machines, or patients themselves” (Hoch 2011). MIT has recently emphasised the same point in the articles “Who will own the robots?” (Rotman 2015) a n d “How t e c h n o l o g y is destroying jobs (Rotman 2013).
Our Approach
There is no other way. We have to advance, as we have begun to do with a PC group in Barcelona, in three ways: improving processes knowledge (Lean Healthcare), innovation in nursing and also in clinical leadership. The main objective has been to obtain the basic requirements of the future use of big data - cognitive computing in PC and to prepare the basis for the acceptance of evolution.
On the other side, we are beginning a project to apply the PHM concept to ageing and dependency - taking care of aged citizens living at home alone. The wellness of aged people in the cities of developed countries is a big clue to healthcare success. Figure 1 synthesises the conceptual model.
Conclusion
Concepts around healthcare systems and the needs and hopes of patients/ citizens are evolving quickly. They are converging and asking for solutions. To simplify, we have the framework, (P HM), t he tools (Big Data and Cognitive Computing) and a model of evaluation (Triple Aim). To advance, we should begin to work in a collaborative model, under a global health approach.
References:
Alderwick H, Ham C, Buck D (2015) Population health systems: going beyond integrated care. London: King’s Fund. [Accessed: 15 July 2015] Available from http://www.kingsfund.org.uk/publications/ population-health-systems
Hoch D (2011) Too many doctors? e-patients.net, 7 March. [Accessed: 15 July 2015] Available from http://e-patients.net/ archives/2011/03/too-many-doctors.html
Institute for Healthcare Improvement (IHI) (2015) IHI triple aim initiative: better care for individuals, better health for populations, and lower per capita costs. [Accessed: 15 July 2015] Available from http://www.ihi. org/Engage/Initiatives/TripleAim/Pages/ default.aspx
Rotman D (2015) Who will own the robots? MIT Technology Review, 118(4): 26-34. [Accessed: 15 July 2015] Available from http://www.technologyreview. com/featuredstory/538401/ who-will-own-the-robots/
Rotman D (2013) How technology is destroying jobs. MIT Technology Review, 116(4): 28-36. [Accessed: 15 July 2015] Available from http://www.technologyreview. com/featuredstory/515926/ how-technology-is-destroying-jobs/
Shortell SM (2013) A bold proposal for advancing population health. Washington, DC: Institute of Medicine. [Accessed: 15 July 2015] Available from: https://www. cdph.ca.gov/programs/cdcb/Documents/ Shortell_bold_%20proposal_July2013.pdf
Weil AR (2014) Our health is global health. Health Affairs, 33(9): 1502. [Accessed: 15 July 2015] Available from http://content. healthaffairs.org/content/33/9/1502.full
World Health Organization (WHO) (2013). The right to health. Fact sheet 323. [Accessed: 15 July 2015] Available from http://www.who.int/mediacentre/ factsheets/fs323/en/
