



HealthManagement, Volume 10, Issue 2 /2008
Author:
Maciej Duszczyk
Institute of Social Policy, Warsaw University, Poland
Email: [email protected]
For the last few years, discussions surrounding employment migration of medical staff have been intense and ongoing in Poland. At times, members of the medical community have used the threat of emigration against the ruling authorities in order to secure salary increases. The issue of threats to the Polish healthcare system ensuing from medical staff emigration was raised during negotiations of Poland’s accession to the European Union. A large part of Polish society itself feared the “brain drain” phenomenon.
In recent weeks, the issue of emigration, however, has lost significance somewhat, because healthcare sector employees have been dealing with other troubling issues. For example, the necessity to be granted approval by hospital directors in order to work in excess of 48 hours weekly, has been a matter of grave concern. This is also related to the complications in the discussions on the working time directive and the necessity to harmonise Polish legislation with the verdict of the European Court of Justice in the Jaeger and Simap cases.
In my opinion, when we are discussing the situation in the Polish healthcare system, which is unfortunately counted among the most poorly remunerated amongst all EU member states, we must consider a much larger problem than migration. There is also the issue of the transition of doctors and nurses to other professions. From the point of view of the Polish healthcare system as a whole, it is preferable for a young medical doctor, who is not content with his/her salary level and opportunities to generate additional incomes, emigrate to another country, where he or she can follow up with their professional career. It is likely that they will return to Poland when their situation has changed, whereas if they were to change profession and then later decide to return to the practice of medicine, they would lack the skills and experience of those who were abroad, but continued to follow medical progress and improve their professional skills.
Let us have a look of the scale of migration of medical doctors after 1st May 2004.
The total number of professionally active medical doctors in Poland amounts to almost 117,000. As indicated by figures from Polish ministry of health, by the end of June 2007 it issued 5851 certificates confirming possession of formal qualifications. This means that 5,04 % of Polish medical doctors in various specialisations were interested in undertaking employment in other EU member states.
An analysis of the existing trends, however, suggests that the number of doctors interested in collecting a certificate authorising them to undertake employment abroad in medical doctor profession has been declining. Between July 2006 and July 2007, the number of issued certificates rose by a mere 737 persons. This was almost two times lower than the figure for the period July 2005-July 2006.
This signifies that a decisive majority of persons who used to link their professional career to employment abroad have already made the step and extinguishing of migration trend is currently very likely. This phenomenon is called the “migration hump” in the migration theory.
The largest number of certificates, taking account of the percentage share in the total number of professionally active medical doctors in a given specialisation, was granted to:
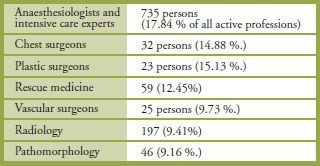
The smallest interest in undertaking employment in other member states is voiced by neonatologists (0,09 %), clinical oncologists (0,25 %) and child neurologists (0,27 %).
The potential employment countries are: Germany, Italy, the United Kingdom, Sweden, Norway, and France. These are traditional emigration countries for Poles, as well as countries that were the first to open their labour markets to Polish nationals. Unfortunately, additional reliable information about destination countries is missing.
At the same time it must be stressed that figures collected on the basis of issued certificates do not perfectly illustrate the scale of emigration. As an example, the system lacks information about persons who collected their certificate but did not decide to leave Poland. Moreover, information is also missing about persons who undertake only additional employment in other member states. This is the case, for example, with anaesthesiologists who sign contracts with a hospital in another member state to provide medical services only one week in a month,without giving up employment in Polish hospitals.
Moreover, many doctors treat the certificate confirming qualifications as a kind of additional policy and security, in cases of a significant deterioration of the situation in the Polish healthcare system. They have decided against emigration and continue to work in Poland, but they do not rule out making a decision to leave in the future.
Paradoxically, the current turmoil in the Polish healthcare system, which is related to the necessity to obtain doctors’ consent for work in excess of 48 hours weekly, will result in higher salaries and can influence the migration potential of doctors. The salary rise will narrow the gap between salaries in Poland and those in states doctors traditionally emigrate to, which will in turn diminish current emigration trends.
In addition to the diminishing differences in salaries, a growing influence on lowering of the migration potential among Polish doctors is exerted by the negative experiences of Polish doctors who decided to leave. Many such doctors frequently perform work below their qualifications and have hampered access to training of most modern medical procedures due to cultural issues, such as language barriers.
In an analysis of the migration of Polish medical doctors one should also take note of the fact that this phenomenon has different consequences from a regional viewpoint. While the fact that a dozen or even several hundred doctors of a
given specialty leave Poland permanently is not a problem from the viewpoint of the entire healthcare system, emigration of even a few doctors from a given region, having e.g. only one or two hospitals, may significantly worsen patients’ access to medical services and force them to travel long way to obtain help.
Although those are not frequent cases, some regional hospitals experienced delays in scheduled surgeries due to absence e.g. of anaesthesiologists.
In conclusion, it must be stated that the emigration of Polish doctors, perhaps excluding anaesthesiologists, has not significantly affected the condition of the Polish healthcare system, but migration processes should continue to be monitored with particular care.
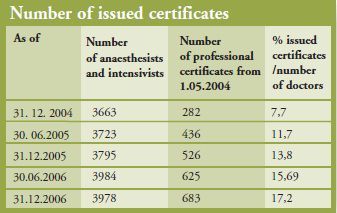
The table above represents the number of doctors-specialists in anaesthesiology and intensive care who are professionally active domestically and the number of issued certificates confirming qualifications to undertake employment in other states.
Presented figures must be treated as a presentation of particular migration potential and not as full information about the scale of migration.
Recapitulation
Migrations of medical doctors only moderately affect the situation of Polish healthcare system. At the same time this phenomenon needs to be monitored, particularly in regional dimension.
The scale of migration depends mainly on the specialty of a given doctor. Anaesthesiologists are the ones most interested in emigration. Paediatricians are those least interested in emigration.
The scale of migration is currently experiencing an extinguishing trend. In 2007 certificates authorising one to undertake employment in other EU member states were collected by fifty percent less doctors than in an analogous period of 2006.
Current legislative changes related to the necessity to implement into Polish law provisions of the working time directive result in significant rises of the salaries of Polish medical doctors. This should be a decisive factor in decisions to give up emigration.