HealthManagement, Volume 14 - Issue 2, 2014
Authors:




Photography, X-rays, Computed Tomography
Using photography (J.A.J. 1869)
and taking plain x-rays are both techniques that were adopted by forensic
scientists or forensic pathologists in a flash, as it appears. As far as plain
x-rays go, first tests by the German physicist Wilhelm Röntgen were done around
November 1885. Not much later, on 25 December 1895 in Montréal, Canada, a male
victim suffered a firearm injury to the leg (Cox and Kirkpatrick 1896). Only
three days later, the first scientific article was submitted by Wilhelm Röntgen
(then in Würzburg, Germany) as a conference contribution, which immediately
made headlines. That conference was the third meeting of the Physical-Medical Society
in Würzburg, Germany. There Röntgen talked about ”a new kind of rays” on 23
January 1896 (Röntgen 1898). With the goal to show the surgeon that was to
remove the bullet of the aforementioned Canadian victim, a plain x-ray was
taken on 7 February 1896 in Montréal, Canada. The patient was sent home ten
days later. A court trial was held later, and the radiographs were presented as
evidence there. Never has a new scientific or technological breakthrough been
so quickly, internationally and universally adopted by the medical and
scientific community (Brogdon 1998; Thali et al. 2011).
Compared to this bush fire type adoption into forensic science, it is surprising to realise that the first adopters used CT (computed tomography) already in 1973 (Richmond 2004), but that CT remained largely unused throughout forensic sciences and medicine. Some scientific papers described methods as we use them in modern Virtopsy®, such as angiographic methods (Karhunen et al. 1989), CT scanning as such (Wüllenweber et al. 1977; Donchin et al. 1994), photogrammetry or 3D surface documentation (Brüschweiler et al. 1997) and MRI (magnetic resonance imaging)( Woodward et al. 1997). However, by 1998 – 25 years later – not one forensic medicine institute had added post mortem CT scanning or other 3D scanning methods to their everyday workflow.
Immediate adoption of a new technique by the whole wide world is not always the instantaneous result. It has been brought about by incentives every now and then though, such as the myoelectric prosthetic arm, whose wider adoption was some what forced upon the Western Bloc by their nemesis, the Russians. At the time, the technology to build myoelectric arms appeared to have been available, but no one seemed to bother with building products that amputees could use (eg, Schlesinger et al. 1919; Battye et al. 1955). In the middle of the Cold War, to the embarrassment of Western countries (Cohen 1955), out of the blue (or so it appeared), the Russians demonstrated a ready-to-use arm dubbed the 'Russian Arm’ (Kobrinski et al. 1950). After that, the Western Bloc countries, to their chagrin, had to send delegations to Russia to ”learn about it” (Sherman 1964). Interestingly, the wider adoption of post mortem forensic imaging was preceded by a similar incentive: one institute charged ahead and just did it.
Virtopsy®
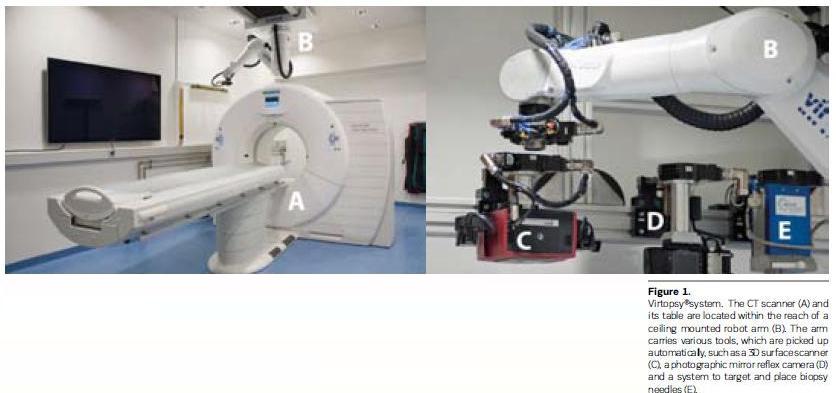
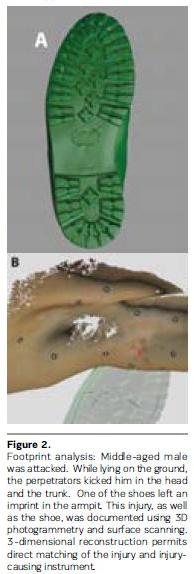
The Virtopsy® research was in part initiated by a high-profile case (see Figure B1.1.3, p. 53 in Thali et al. 2009). The first body scans were started by our group in 1999, using project names such as ‘digital autopsy’ or ‘scalpel-free autopsy’. With that, the Virtopsy® project was born (Dirnhofer 2001). This project was not the first attempt to use CT or MRI post mortem scanning worldwide (see references above), but it was undoubtedly the first to incorporate a broad range of technologies such as CT, MRI, biopsies (see Figure 1 overleaf) for an overview of the Virtopsy® system also containing a Virtobot®), 3D surface scanning (see Figure 2 for an example of surface data evaluation and injury matching), while also examining as many cases as possible over an extended period of time and in a systematic manner. A considerable number of traditional forensic pathologists expressed a ‘dislike’ for these new methods, but at the very same time this immediately was news all over the globe.
The targeted activity of the Virtopsy® research group around Richard Dirnhofer was widely communicated in conferences after 1999. The systematic approach and broad scope were unprecedented (eg, gunshot focused research (Thali, Yen, Schweitzer et al. 2001a), sharp force trauma (Thali, Schwab et al. 2001; Schweitzer, Yen, Thali et al. 2001a , Thali, Braun et al. 2001), heat and strangulation (Thali, Yen, Schweitzer et al. 2001b), post mortem interval estimation (Ith et al. 2001; Scheurer et al. 2001), skull and brain injury (Yen et al. 2001), heartfocused research (Schweitzer et al. 1998; Schweitzer, Schaepman et al. 2001; Schweitzer, Yen, Thali et al. 2001b) and 3D surface pattern matching (Brüschweiler, Braun, Thali et al. 2001a; 2001b)). Subsequently, results were made available also in compiled form (Thali et al. 2002; Thali et al. 2003; Thali et al. 2009).
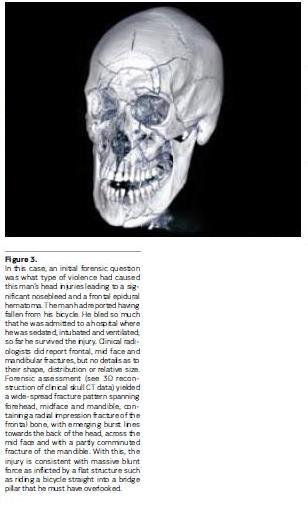
Virtopsy® subsequently developed into a multi-tool documentation and analysis research project (Thali et al. 2009), combining 3D body surface imaging methods with merged CT and MRI data and 3D shape analysis (Thali et al. 2005; Buck, Naether et al. 2007; Buck, Albertini et al. 2007; Ebert et al. 2010; Schweitzer et al. 2013; Röhrich, et al. 2012). The application of multidetector or multislice (Ohnesorge et al. 1999) CT and MRI found continued interest (Aghayev et al. 2005; Bolliger et al. 2005; Jackowski et al. 2005; Yen et al. 2007; Buck et al. 2009; Ruder et al. 2012) also for problems specific to clinical forensic medicine (Yen et al. 2005; Yen et al. 2007), then for high-resolution micro-CT (Thali, Taubenreuther et al. 2001; Thali et al. 2003) and micro-MRI (MR microscopy) (Thali et al. 2004), magnetic resonance spectroscopy (time-of-death determinations) (Ith et al. 2002; Scheurer et al. 2005; Ith et al. 2011), image-guided percutaneous biopsy (Aghayev et al. 2007; Aghayev et al. 2008; Ebert et al. 2010; Ebert et al. 2012; Ebert et al. 2014), post mortem angiography (Jackowski et al. 2005; Grabherr et al. 2006; Gyax and Grabherr 2009; Gyax and Grabherr 2010; Grabherr and Gyax 2012; Gyax et al. 2013; Ross et al. 2008), post mortem identification (Jackowski e t a l. 2 006; P faeffli et al. 2007), post mortem ventilation (Germerott et al. 2010; Germerott et al. 2012), and non-invasive tool and data display control such as the integration of a Kinect camera (Ebert et al. 2013; Ebert et al. 2012) or 3D printing and rapid prototyping (Ebert et al. 2011). Added value for the conventional autopsy results from improved planning and better diagnostics. Some concise advantages are the identification and incorporation of bone bruises into accident reconstructions (Buck et al. 2009), the identification of gas (relevant in diving-related deaths (Plattner e t a l. 2 003; O zdoba e t a l. 2005; Wheen and Williams 2009)), the ability to identify pathology in decaying tissue (that can be difficult if not impossible to handle manually at dissection (Thali et al. 2003; Takahashi et al. 2013)), the ability to extract and use information related to (chemical) material composition (Persson et al. 2008; Alkadhi and Leschka 2013), documentation of medical installations (Oesterhelweg et al. 2009) and exploitation of digital data for reconstructive purposes (Thali, Braun et al. 2005; Buck et al. 2007; Weilemann e t al. 2008; Röhrich et al. 2012). Furthermore, advances in usage of reconstructive aspects of 3D CT reconstructions have led to routine integration of forensic aspects into clinical forensic medicine (see Figure 3). In the last 15 years, there have been numerous publications on forensic imaging (Baglivo et al. 2013). The significant technological step in forensic medicine can be described as the advancement from the ‘forensic camera obscura’ to ‘Star Treklike Virtopsy® and VirtobotQR technologies’ (Thali et al. 2009). However, the core aim of the Virtopsy® project is not to eliminate the classical approaches, but to implement imaging techniques in forensic medicine that are at the level of the current technology (see figure 3).
Current Status and Outlook
Currently, there are a few centres
that offer 3D model testing (such as the Institute of Forensic Medicine in
Bern, Switzerland (Thali et al. 2002; Bolliger et al. 2010)) and 3D scanning
(centres in Bern and Zürich, Switzerland) (Buck et al. 2007)). Post mortem
imaging following the Virtopsy® approach is increasingly being employed around
the world. This was apparent already a few years ago (Oesterhelweg and Thali
2009), while in the meantime major implementations seem to be underway at least
in the United Kingdom as well as the United States of America (Edwards 2009).
In forensic pathology, the following workflow emerges as standard: 3D surface scanning to document body surface and injuries in 3D and CT scanning to document any bone injuries and gross pathology.
The forensic imaging approach has the following potential:
• Recorded data are observer-independent, archived for later retrieval and can be reviewed by others or subjected to new analytical techniques, and possibilities for teleradiopathology are opened (second opinion).
• Material analysis is possible or approximated (Alkadhi and Leschka 2013).
• Scanning is non-destructive and does not tamper with the forensic evidence.
• Data provide a 1:1 match to the body and correct 3D geometry in xyz-axes or spatial documentation, which can be used as the basis of 3D scientific reconstruction.
• The approach provides an alternative or additional examination that ‘sees’ different aspects of the body, as CT ‘sees’ with x-rays and MRI ‘sees’ chemical distributions (Jackowski et al. 2006).
• Difficult-to-examine body areas can be examined (eg, face, neck, spine, pelvis).
• The technique could be considered in cultures and situations where autopsy is not tolerated by religion or is rejected by family members (e.g., psychological reasons) (Goodman et al. 2011; Cannie et al. 2012).
• Bodies contaminated by infection toxic substances, radionuclides, or other bio-hazards (i.e., bioterrorism) can be subjected to touch-free examination (more detailed requirements see eg, (Nolte et al. 2004)).
• 2D and 3D post-processing are provided for visualisation of the findings, which may be particularly relevant for people not present during the examination.
• A case’s presentation in court may be understood better, more easily and in a more matter-of-fact way (Ampanozi et al. 2012).
• A new strategy option is introduced, specifically, examining a case stepwise. This is achieved by first doing an external inspection, then possibly a CT scan, then reading the data, then possibly an MRI, again evaluating the data, and ultimately deciding whether to do or not do to an autopsy. Thus, cases can be examined in a way that optimises quality and cost.
The forensic imaging approach (when applied alone) includes the following disadvantages:
• CT scanners have limited soft tissue contrast.
• Organ colours cannot be visualised (so that, eg, inflammation, tumour, scars, etc. can be hard to discriminate). It is necessary for those interested in the future of forensic imaging to cooperate on an international basis at a high level, exchanging and sharing research results and acquired experience. There is a need for the education and teaching of highly trained professionals, which requires both financial support and enthusiasm. In light of global terrorism, it might be possible for the forensic field to acquire grant-based financing. Government institutions such as the United States Department of Homeland Security are already starting to consider funding research about this topic. As such, financial support seems more possible than in previous years. For that purpose, the International Society of Forensic Radiology and Imaging (www.isfri.org) was founded in 2011. Additionally, in 2012, the Journal of Forensic Radiology and Imaging (www.jofri.net) was born. A new “Forensic Radiology” sub-discipline has opened up, bridging the worlds of Forensics and Radiology.
Because the Virtopsy® multi-tool approach will create a process of change in forensic medicine over the subsequent decades, teaching will be an important and core topic over the next few years. C SI television series have resulted in an increased interest in the forensic sciences (Schweitzer and Saks 2006; Knoblauch 2012). With the adoption of new imaging techniques, forensic sciences have indeed opened up a new area of research and a new area for service options.