HealthManagement, Volume 16 - Issue 1, 2016
Quality accreditation can provide a sustainable competitive advantage to healthcare businesses if they build their strategy around creating infrastructure, policies and processes compliant with the Indian National Accreditation Board for Hospitals & Healthcare Providers (NABH ) standards. The standards promote adherence to global best practices of healthcare delivery, and there are detailed guidelines on measuring performance of hospitals on pre-defined quality indicators (nabh.co/standard.aspx). Accreditation requires an organisational culture change, which needs to be sustained for a longer period of time. A culture developed on the bedrock of quality care and patient safety will provide utmost quality assurance to patients and the community. Patients have become more aware about accreditation, and they are basing their choice of hospital on whether the hospital is accredited or not.
NABH Standards for Hospitals
The 10 chapters reflect two major aspects of healthcare delivery, ie patient-centred functions (Chapters 1-5) and healthcare organisation-centred functions (Chapter 6-10), as follows:
Patient-Centred Standards
- Access, assessment and continuity of care (AAC);
- Care of patients (COP );
- Management of medication (MOM);
- Patient rights and education (PRE );
- Hospital infection control (HIC);
Organisation-Centred Standards
- Continuous quality improvement (CQI);
- Responsibilities of management (ROM);
- Facility management and safety (FMS);
- Human resource management (HRM);
- Information management system (IMS).
Aim
This project aimed to conduct self-assessment against NABH accreditation standards, gap analysis and action planning at a leading multispeciality corporate hospital of north India. Secondary objectives were to:
- Study the efficient functioning of the Hospital, area-wise
and department-wise to ascertain that the standard operating procedures are
being followed in an accurate and effective manner.
- Ascertain the organisation’s preparedness and commitment to
quality goals and conformance to accreditation standards.
- Understand the effectiveness of employee satisfaction indicators
on implementing NABH processes.
- Suggest effective solutions through action planning that the
hospital can adopt to bridge such gaps.
Methods
This was an observational study that involved collection of primary data via structured observation tools, staff and patient interviews, studying the standard operating procedures (SOP s) of the department and putting the observations on the audit tool. The areas that were considered and studied empirically were:
- Patient care areas: outpatient department (OPD ),
inpatient department (IPD ), day care centre, operating theatres, intensive
care units.
- Support areas: nursing stations, diagnostics (laboratory and
radiology), pharmacy;
- Ancillary service areas: central sterile supply department
(CSSD ), food and beverage, laundry, engineering services, biomedical
engineering, medical gases, biomedical waste management (BMWM) and medical
records department (MRD );
- Administrative areas: executive offices and other
nonrevenue generating units;
 Scoring Pattern
Scoring Pattern
- Score 10/10: 100% compliance to the requirement.
- Score 5/10: Partial compliance to the requirement (if any of
the sample is found to be non-compliant out of total samples selected).
- Score 0/10: Non-compliance to the requirement.
- NA : Not applicable.
Findings and Data Analysis
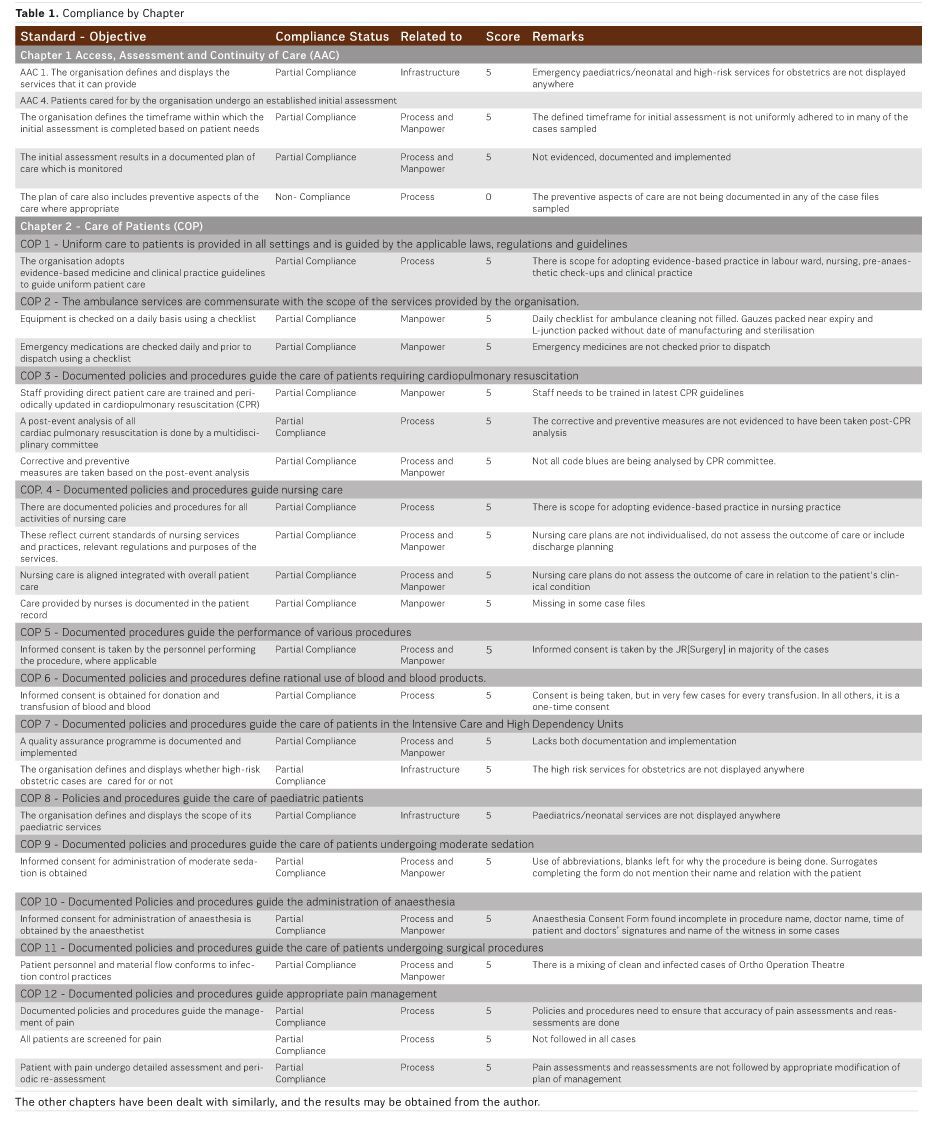
The following tables show partial and non-compliances with remarks about the actual observations of the gap for selected standards.
Gaps in Compliance
Infrastructure-related gaps form the lowest percentage (seven percent) followed by manpower gaps (thirty-three percent). The highest percentage of non-conformances (sixty percent) is process-related. Some nononformances are both process-related (lack of documentary evidence) and manpower related (lack of implementation). These have been added separately under both headings thus increasing the total number to 134.
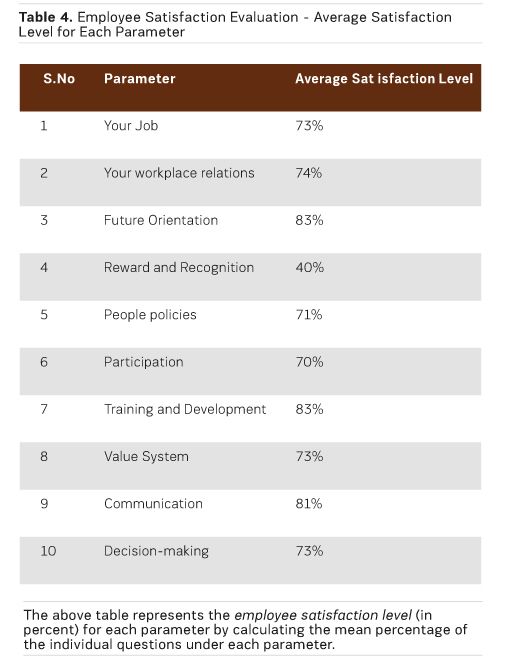
Employee Satisfaction Evaluation
Table 4 shows the employee satisfaction level (in percent) for each parameter by calculating the mean percentage of the individual questions under each parameter. The overall employee satisfaction rate was 73 percent.
Discussion
A thorough analysis of areas of non-compliance to the NABH standards revealed that infrastructure-related gaps are 7 percent, manpower gaps are 33 percent and process-related gaps the highest percentage at 60 percent. Overall compliance observed is 89.9 percent and non-compliance is 10.1 percent. The upside to these findings is that the improvements can be made with only a little investment of financial resources since the non-conformances that require infrastructural modifications and enhancements form the lowest percentage.
Next Steps
The processes need to be clarified and strengthened at the top-level first and then handed down to the staff for effective implementation. The core team and sub-committees will include members from lower and middle management positions to translate the actual flow of activities into SOPs. This will help to minimise the difference between achievable and absolute levels of performance. The ideal approach is to seek suggestions from front-line staff on policy formulation and revision since they are the ones who practically face the actual difficulties in on-the-ground implementation. However, this does not cast any form of doubt on the successful process of the time-tested patient care system that has been in place in this hospital since its inception. NABH is merely an enhancement of these processes to conform to national and international standards.
Conclusion
It can be stated with confidence that these enhancements can be made as per the NABH requirement details outlined in the NABH Manual. The study findings have indicated a strong positive association between the NABH process implementation and employee satisfaction. Though the overall percentage of employee satisfaction is calculated to be 73 percent, the employees at this hospital see conforming to standards as an additional burden. Since the staff has to actively participate in the implementation of both patient-centred and organisation-centred standards, it is perceived as an imposed responsibility rather than a voluntary commitment to quality.
Key Points
- How can hospitals assess their quality dimensions.
- Ten chapters in the articles reflecting both the patient-centred
functions and healthcare organisation-centred functions have been demonstrated.
- Study ascertains the organisation’s preparedness and
commitment to quality goals and accreditation
- standards.
- Understand the effectiveness of employee satisfaction indicators
on implementing the accreditation
- processes.
