HealthManagement, Volume 14 - Issue 2, 2014
Author:
CT Radiation Exposures in Pediatric Patients (no. 3)
Paediatric patients are inherently more sensitive to the effects of ionising radiation than are adults. While the risk has always been hard to quantify, newly published empirical studies add to the evidence that exposure to ionising radiation from diagnostic imaging at a young age can increase a person’s risk of developing cancer later in life. (See the figure 1.)
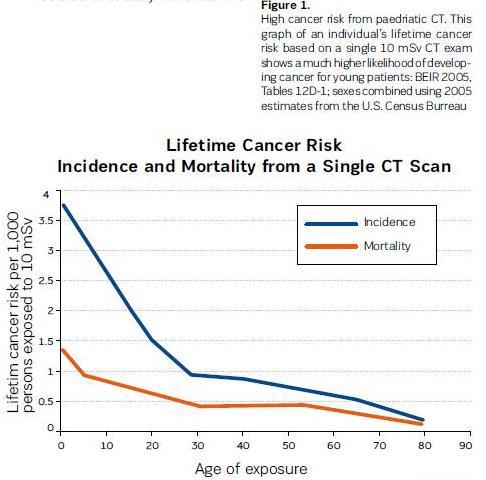
CT scans make use of ionising radiation, which can damage DNA and other cellular structures. This in turn can lead to an increased risk of cancer. The potential for such damage is estimated by calculating the effective dose. The greater the effective dose, the greater the likelihood of harm. The effective dose delivered by CT is among the highest in diagnostic radiology. The level of risk is subject to considerable debate, the calculations being largely based on data collected following the atomic bomb detonations during World War II. However, retrospective studies are now being published that indicate an increased risk of future cancers for children exposed to CT (Matthews et al. 2013; Pearce et al. 2012).
Using safer diagnostic options when appropriate
Actions that healthcare providers can take to minimise a child’s exposure to high doses of ionising radiation include using safer diagnostic options when appropriate, in consultation with a radiologist:
- MRI is considered the preferred choice for diagnosing problems such as ligament and tendon damage, spinal cord injuries, and brain tumours.
- Ultrasound is still effective at revealing the presence of soft-tissue abnormalities. Because ultrasound has difficulty imaging through bone and air-filled lungs, this technology is most commonly used for scanning abdominal organs.
- X-rays. Because radiography, including digital radiography, uses substantially lower radiation dose than CT, it should be considered as an alternative to CT when diagnosing children. Some new digital techniques, such as digital tomosynthesis, are becoming available that improve the amount of information available with radiography without greatly increasing the radiation dose.
Avoiding repeat scanning
Obtaining the existing images from previous scans can greatly reduce the need for repeat scans, and thus decrease the amount of radiation paediatric patients are exposed to over the course of their diagnosis and treatment.
Following the ALARA principle
Care must be taken to use a dose that is ‘as low as reasonably achievable’ (ALARA) to acquire the desired diagnostic information. This can include avoiding the use of ‘adult size’ doses on children, as well as minimising radiation exposures to parts of the body that are beyond the area of interest.
Recommendations
- Implement appropriate use criteria for determining whether alternative methods could be used when urgency or symptoms do not necessitate CT. A radiologist should be consulted to determine the best method.
- Before initiating a new CT study, try to identify whether a scan has already been performed on the patient, perhaps at another institution. Obtain the results of these scans if possible, and consider whether they are sufficient for diagnosis and treatment without the need for further scanning.
- When CT has been determined to be necessary:
- Use the ALARA principle to minimise radiation exposure.
- Customise scanning protocols to the needs of paediatric patients— that is, recognise that settings designed for adults are not appropriate for children.
- Take care to avoid beyond boundary scanning (i.e., unnecessarily delivering the dose beyond the anatomical area of interest) and overexposure.
- Update your scanning protocols as necessary to reflect the latest guidance from professional organisations such as the American College of Radiology and the American Association of Physicists in Medicine.
Risks to Paediatric Patients from ‘Adult’ Technologies (no. 8)
Healthcare technologies are often developed with the needs of adult patients in mind, leaving clinicians with little choice but to rely on ‘adult’ technologies in the diagnosis and treatment of paediatric patients. Due to their smaller size and ongoing physiologic changes, children may suffer adverse effects when subjected to adult-oriented healthcare techniques. Unfortunately, paediatric-specific devices can be slow to reach the market because of the small numbers of patients available to study, the devices’ high-risk nature, and high development costs. Healthcare personnel must exercise particular care when this is necessary.
Discussion
The following are just a few examples of how the care of pediatric patients can be compromised when applying ‘adult’ healthcare technologies:
Radiation exposure hazards
E xposure to ionising radiation such as that used in CT and x-ray imaging has been associated with an increased cancer risk. Because they are still developing, children are especially susceptible to long-term damage from radiation exposure. To compound this problem, using adult scanning techniques on children can expose them to an unnecessarily large ‘adult’ dose and can potentially expose regions of the body outside the area of interest (see hazard number 3 in this year’s list).
Electronic health records
A healthcare facility’s EHR may not be configured to optimally support the care of children. For example, the system may not facilitate the recording and review of important paediatric-specific data, such as vaccinations, or may not allow both height and weight to be viewed on the same screen, which in turn can contribute to vital information being overlooked. To bridge the gap between the functionality present in most currently available EHRs and that needed to better support children’s healthcare, the Agency for Healthcare Research and Quality (AHRQ) recently announced the development of the Children’s HER Format. The Format provides information to help EHR developers optimise their systems for the care of children, as well as criteria to help facilities select an EHR that supports children’s healthcare needs.
Medication dosing errors
Children, because of their small size, are particularly susceptible to adverse consequences from incorrect dosing. This susceptibility to harm, coupled with the use of technologies that aren’t optimised for paediatric patients, can lead to tragic results. A device as simple as a scale can contribute to significant harm. In one report to ECRI Institute PSO, a mix-up involving the use of pounds versus kilogrammes to record weight contributed to the death of an infant. In a similar incident, a toddler’s weight was measured to be 25 lb (11.3 kg), but was mistakenly recorded in the EHR as 25 kg. Calculating the dose using the incorrect weight led the physician to prescribe a drug at about twice the desired dose. Fortunately, the child’s mother recognised the error before the child experienced significant adverse effects (Bokser 2013). Even advanced technologies intended to help decrease medication errors are fallible. For example, the authors of a 2012 study identified CPOE systems as an enabler of tenfold medication errors in paediatric patients. The authors cited the “overriding of recommendations, ignoring of alerts, and the inability of CPOE to recognize certain tenfold underdoses” as contributing factors, and they noted the need for CPOE systems to be “designed in a standardized fashion that incorporates paediatric-specific dosing logic” (Doherty and McDonnell 2012).
Recommendations
• When assessing medical technologies and supplies for purchase or use, consider the extent to which the device, system, or accessory has been developed with the needs of paediatric patients in mind. For example:- When selecting an EHR, consider the extent to which the system complies with AHRQ’s Children’s EHR Format. (see http://healthit.ahrq.gov/health-it-tools-andresources/childrens-electronichealth-record-ehr-format.)
- Use electronic medication prescribing (e-prescribing) systems that include such features as child-specific medication libraries, normative references, and child-specific weight-based dose calculations and alerts.
- For infants and children, use scales that can be set to provide weights in kilogrammes only, and verify that the scales are clearly labelled as such.
- Whenever possible, use paediatric-specific technologies rather than using adult-oriented technology off-label or employing workarounds.
- If obtaining paediatric-specific technology is not an option, investigate whether an available device can be safely and effectively used on children. Alternatively, ask if the vendor can refer you to current users of the technology who have implemented the system in a manner that addresses the needs of paediatric patients.
- Consider identifying a paediatric technology safety coordinator to assess both the adult-oriented technologies and the adult-paediatric hybrid technologies that are being used on pediatric patients at your facility. Responsibilities may include:
- Identifying devices, accessories, or systems that are appropriate for only a certain range of patients (e.g., adults but not children)
- Identifying devices, accessories, or systems that must be used in a specific configuration to safely accommodate paediatric patients (e.g., restricting the upper flow rate for infusion pumps)
- Where appropriate, clearly labelling any such devices
- Educating staff about unique safety considerations or methods of use that are required when working with paediatric patients
- Establishing protocols for setting medical device alarms to levels that are appropriate for paediatric patients and periodically verifying that these protocols are being followed.
Data Integrity Failures in EHRs and Other Health IT Systems (no. 4)
Reports illustrate myriad ways that the integrity of the data in an EHR or other health IT system can be compromised, resulting in the presence of incomplete, inaccurate, or out-of-date information. Contributing factors include patient/data association errors, missing data or delayed data delivery, clock synchronisation errors, inappropriate use of default values, use of dual workflows (paper and electronic), copying and pasting of older information into a new report, and even basic data entry errors. Some of the mechanisms by which the information in an EHR or other health IT system could become compromised:
- Patient/data association errors
- Missing data or delayed data delivery
- Clock synchronisation errors
- Inappropriate use of default values
- Maintaining hybrid (paper and electronic) workflows
- Copying and pasting older information into a new report
- Data entry errors, e.g. entering incorrect information, selecting wrong item from a drop down menu, or entering information in the wrong field.
Recommendations
- Before implementing a new system or modifying an existing one, assess the clinical workflow to understand how the data is (or will be) used by frontline staff, and identify inefficiencies as well as any potential error sources.
- Test, test, and retest
- Phase out paper.
- Provide comprehensive user training.
- Provide support during and after implementation.
- Facilitate problem
Neglecting Change Management for Networked Devices and Systems (no. 7)
The growing inter relationship between medical technology and IT offers significant benefits. However, one underappreciated consequence of system interoperability is that updates, upgrades, or modifications made to one device or system can have unintended effects on other connected devices or systems. ECRI Institute is aware of incidents in which planned and proactive changes to one device or system—relating, for example, to upgrading software and systems, improving wireless networks, or addressing cybersecurity threats—have adversely affected other networked medical devices and systems. To prevent such downstream effects, alterations to a network or system must be performed in a controlled manner and with the full knowledge of the personnel who manage or use the connected systems. Unfortunately, change management—a structured approach for completing such alterations—appears to be an underutilszed practice.
Discussion
In today’s hospitals, initiatives that once may have been considered ‘IT projects’ must instead be viewed as ‘clinical projects that require IT expertise.’ Software upgrades, security patches, server modifications, changes to or replacement of network hardware, and other system changes can adversely affect patient care if not implemented in a way that accommodates both IT and medical technology needs. Consider the following examples:
- An ECRI Institute member hospital described an incident in which a facility-wide PC operating system upgrade caused the loss of remote-display capability for its foetal monitoring devices. The facility had configured its foetal monitoring system so that nurses could view the output on a PC located outside the patient’s room. However, these displays became nonfunctional when the IT department pushed out a Windows 7 upgrade to the computers connected to the network. The PC application that allowed the display of the foetal monitor information was not compatible with Windows 7.
- Another member hospital experienced problems displaying foetal monitor data on workstations at the nurses’ station following an IT change. In this case, the problems began after the IT department moved the obstetrical data management system server offsite. No verification testing was performed to ensure continued performance after the change.
- An update to the firmware for the wireless access points at a member hospital caused the loss of wireless functionality for some of the facility’s medical devices. Some physiologic monitors, for example, required a wired connection for months until a fix could be implemented.
- A recent article describes an incident in which an EHR software upgrade resulted in changes to certain radiology reports, causing fields for the date and time of the study to drop from the legal record. The fields remained in the screen display, so staff using the EHR system did not detect the change to the legal record. (See the June 2013 edition of ECRI Institute’s Risk Management Reporter for details.) Appropriate change management policies and procedures, as outlined in the recommendations below, can help minimise the risks. Just as important, however, is to cultivate an environment in which IT, clinical engineering, and nursing/medical personnel (1) are aware of how their work affects other operations, patient care, and work processes—particularly clinical work processes—and (2) are able to work together to prevent IT-related changes from adversely affecting networked medical devices and systems.
Recommendations
Effective approaches to change management include the following:
- Facilitate good working relationships among departments that have a direct responsibility for health IT systems, medical technology, and change management. Involve the appropriate stakeholders when changes are planned.
- Maintain an inventory listing the interfaced devices and systems present within the institution, including the software versions and configurations of the various interfaced components.
- Take steps to ensure that changes are assessed, approved, tested, and implemented in a controlled manner. ECRI Institute recommends that, when possible, the changes and associated system functionality be tested and verified in a test environment before implementation in a live clinical setting. Change management applies to a variety of actions, including hardware upgrades, software upgrades, security changes, new applications, new work processes, and planned maintenance.
- Evaluate the facility’s policies and procedures regarding change management. Care should be taken to determine how technology decisions involving health IT systems, medical devices, and IT networks can affect current operations, patient care, and clinician work processes.
- Develop contract wording that is specific to change management. For example, contracts with vendors should require the necessary documents (e.g., revised specifications, software upgrade documentation, test scenarios) to be provided to the appropriately designated staff member(s) to facilitate change management. Stipulating that vendors provide advance notice of impending changes can give healthcare facilities time to budget and adequately plan for those changes.
- Ensure that any system updates do not jeopardise processes to maintain the privacy of patients’ protected health information and the security of records with that information.
- When making changes to interfaced systems, closely monitor the systems after the change is made to ensure their safe and effective performance.
- Provide frontline staff members a point of contact for reporting problems related to change management and health IT systems. Education, training, and good escalation procedures (so that reports reach someone who can respond if the first person is unavailable or lacks the necessary competence) can help to ensure that problems are addressed with the appropriate urgency. In addition, consider applying risk management principles to change management as discussed in the IEC 80001-1 standard, Application of Risk Management for IT-Networks Incorporating Medical Devices— Part 1: Roles, Responsibilities and Activities.