




A recent trial involving all hospitals in London, U.K., reports no disparity in survival at 30 days in patients with resuscitated cardiac arrest who were transported by ambulance to a cardiac arrest centre or the nearest emergency department. These findings were presented during a Hot Line session at the ESC Congress 2023.
Sudden cardiac arrest is accountable for one out of every five deaths in industrialised countries. Measures such as cardiopulmonary resuscitation by laypeople, early defibrillation, and advancements in in-hospital management have improved the prognosis after out-of-hospital cardiac arrest (OHCA). However, despite these improvements, only one in ten OHCA patients survive until discharge from the hospital.
Cardiac arrest centres offer targeted critical care, acute cardiac treatment, radiology services, and appropriate neuroprognostication beyond what conventional emergency departments can provide. Non-randomised studies suggest that transporting OHCA patients to specialist cardiac arrest centres via ambulance enhances survival rates, driving efforts to prioritise the treatment of cardiac arrest victims in these facilities.
The ARREST trial investigated whether the expedited transfer of OHCA patients to a cardiac arrest centre would reduce mortality compared with delivery to the nearest emergency department. The study also examined potential differences in neurological outcomes between the two approaches.
Successfully resuscitated OHCA patients without ST-elevation on their post-resuscitation electrocardiogram (ECG) were randomised pre-hospital to 1) rapid delivery to a cardiac arrest centre or 2) delivery to the nearest emergency department. In the intervention group, paramedics alerted the designated cardiac arrest centre before arrival.
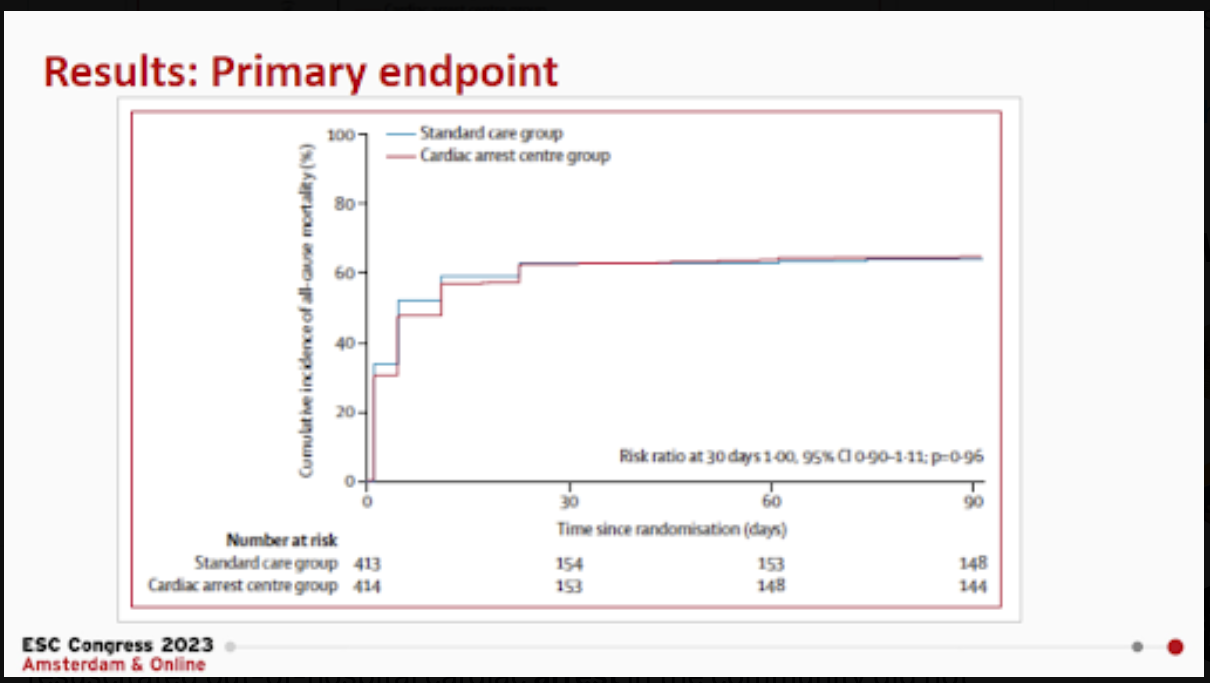
The primary endpoint of the study was all-cause mortality at 30 days in the intention-to-treat population. Secondary endpoints included all-cause mortality at three months and neurological outcomes at discharge and three months.
A total of 862 patients were enrolled, with 431 (50%) randomly assigned by London Ambulance Service paramedics for expedited transfer to a cardiac arrest centre and 431 (50%) to standard care.
The primary outcome of 30-day all-cause mortality occurred in 63% of patients in the cardiac arrest centre group and 63% in the standard care group. There was no significant difference in the secondary endpoint of three-month all-cause mortality between the two groups. Neurological outcomes were similar at hospital discharge and three months for both the groups.
Dr.Tiffany Patterson, study author affiliated with Guy's and St Thomas' NHS Foundation Trust in London, UK, stated that the findings of this study do not support transportation of all patients to a cardiac arrest centre after resuscitated cardiac arrest. These centres are high-resource facilities. If delivering patients to such centres for multiple interventions does not improve overall survival, reallocating these resources to other areas would be more effective. Moreover, not taking all cardiac arrest patients to these centres opens up capacity for other emergency work, including trauma, ST-elevation myocardial infarction, and acute aortic dissection, which requires high-dependency beds and the specialised expertise available in these centres.
Source: ESC Congress 2023
Slide and Image Credit: ESC Congress 2023



