



HealthManagement, Volume 2 - Issue 2, Winter 2008
In the twenty years since the demise of the Soviet Union, Latvia has transformed itself, gaining its independence not only politically but also in medicine. While formerly, research, innovations and financial investments were concentrated in Moscow and less in the Baltic States, in present times Latvia is a member of the European Union, is independent, and its citizens can make their own decisions and control their own future.
The main challenges for us during the last 20 years have been to
reduce the prevalence and incidence of cardiovascular disease and to decrease
cardiovascular mortality. The burden of cardiovascular mortality and morbidity
is very high in Latvia. According to epidemiologic data, cardiovascular disease
emerges as the leading cause of mortality in Latvia (54.6% from total deaths in
2007) (Ministry of Health of the Republic of Latvia 2007).
Modernising Cardiology Services
The first step was the introduction of modern diagnostic and
management methods, for example, interventional cardiology. Due to insufficient
funding in healthcare during the nineties, modern facilities and services were
only accessible in the Latvian Centre of Cardiology at Pauls Stradins Clinical
University Hospital. Expanding modern medical tools across the country and
improving the availability of services were a key factor. Then, in order to
evaluate healthcare quality and accessibility the national registry of acute
coronary syndrome was introduced in 2001.
Interventional Cardiology
The most significant advance in cardiology, was during the beginning of the interventional cardiology era in 1990, when myself and Andis Dombrovskis carried out our first angioplasty in Latvia. For the first 15 years the Latvian Centre of Cardiology was the country’s only existing interventional centre. Nowadays, it is one of the largest interventional cardiology centres in Europe, where the newest methods are used and research carried out. Since 2004, regional centres of interventional cardiology have been launched, with three interventional cardiology centres in capital city Riga and two in regional hospitals.
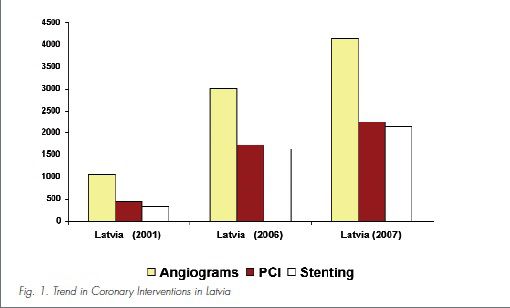
The number of percutaneous coronary interventions (PCI) per
million inhabitants in Latvia continues to increase. In 2007, we had 1,736
percutaneous coronary interventions (PCI) which corresponds to a four-fold
increase since 2001 (see fig. 1). The mean number of PCIs per million in Europe
in 2005 was 1,601 (Praz et al. 2008). Active usage of intravascular diagnostic
devices (intravascular ultrasound, OCT, virtual histology) and modern PCI
modalities (LM interventions with cutting balloon pretreatment) have been
investigated at the Latvian Centre of Cardiology and introduced into practice (Erglis
et al. 2007). Since 2001, the major non-coronary procedures were introduced at
the centre, including alcohol ablation for septal hypertrophy, percutaneous
closure of atrial septal defect, patent foramen ovale or ductus arteriosus and
percutaneous treatment of aortic coarctation. Recently, we have started to perform percutaneous valvuloplasties and stem
cell intracoronary delivery is also now on our list of offered treatments.
The National Registry of Acute Coronary Syndromes (ACS)
The National Registry of Acute Coronary Syndromes (ACS) was developed to pinpoint if knowledge coming from clinical trials is being properly applied in different hospitals in our country. The aim of this registry was to identify changes in therapeutic approaches and outcomes of ACS patients in Latvia. The study sample consisted of 7,232 patients with ACS in year 2001 and 9,881, 8,261 and 7,777 patients with ACS admitted across all the country in years 2005, 2006 and 2007 respectively. Randomised trials comparing thrombolysis and PCI show that primary PCI results in lower in-hospital mortality, rate of the reinfarction and stroke (Grines et al. 1993). However, its availability is limited and a large proportion of patients are reperfused with thrombolysis (Morrow et al. 2005). Although we have at least oneinterventional centre within a coverageradius of 100km in Latvia, a 24-hour service is available only at our centre. Therefore most other Latvian hospitals are still using thrombolysis.
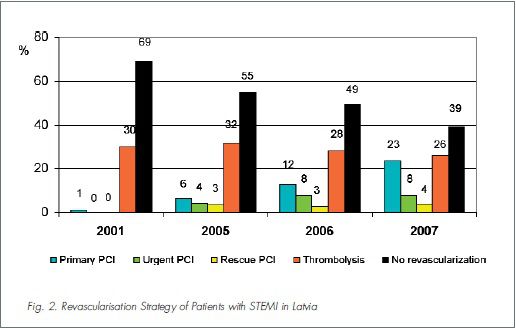
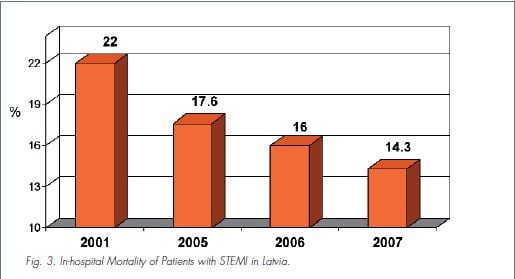
Since 2001, the use of fibrinolytic therapy has slightly decreased, and the incidence of primary PCI has increased (see fig. 2). Based on ACS registry data, in 2001, the first Latvian National Guidelines of Acute Coronary Care were developed by the Latvian Society of Cardiology and were implemented in practice. It has resulted not only in changes of management but also in improvement of clinical outcomes, for example, in-hospital mortality (see fig. 3). One of the main areas where more development is required is in the education of doctors – especially general practitioners and cardiologists. All Latvian interventional cardiologists are trained at excellent interventional centres in different countries like the United States, Australia, France, Netherlands, Germany, and Italy. It is essential to admit that we have trained not just interventional cardiologists but also echocardiographers, intensive care specialists and functional clinicians.
Primary Prevention
For years, cardiology has focused primarily on treatment via drugs
and interventions, but now the focus is turning more towards prevention,
especially primary prevention. In order to participate in this initiative, the Latvian
Society of Cardiology delivers different educational programmes for society using
mass media. For example, we coordinated different advertisements on TV and radio
with information about dislipidemia, smoking, overweight issues, and hypertension
as risk factors for cardiovascular disease to educate the public.
Also, we have developed “heart health” rooms in outpatient
clinics, where patients can come and measure their blood pressure, cholesterol
levels as well as get specialist consultations. We have introduced programmes
that promote heart health in school
children. We have measured body weight
and blood cholesterol levels in children in schools and promoted healthy diet
and physical activity to raise awareness amongst the next generation.
Conclusions
Cardiology has changed dramatically in the last two decades, the result of which is a trend in decrease of cardiovascular mortality and morbidity. We have achieved enormous progress in interventional cardiology ensuring large volumes of coronary interventions maintaining quality, which always have been our priority. Our cardiologists, primary care specialists and finally our society is reasonably better educated than a few years ago.
