



HealthManagement, Volume 2 - Issue 1, Spring 2008
Coronary artery disease (CAD) is the leading cause of mortality in the industrial world. Cardiac imaging is essential to establish the diagnosis and severity of CAD and to determine the potential risk of future cardiovascular events. In patients with suspected CAD, evaluation of patient history will reveal the presence of cardiac risk factors and typical symptoms. An ECG should be performed in all patients with suspected CAD. This article explores the different methods for imaging cardiac diseases, reviews the pros and cons of each method.
Echocardiography
This painless, non-invasive test uses sound waves to create 2D
images of the cardiovascular system. New systems also produce 3D images. With
the help of Doppler ultrasound it also produces information about the velocity
of blood flow in the heart and measures heart valve function. A transducer is
placed on the chest wall of the patient in order to transmit and receive
acoustic signals. The size of all four heart chambers is measured and left and
right heart chamber function is assessed. Echocardiography is simple, can be
performed quickly, and is radiation- and risk-free. Echo machines are mobile
and can hence be used everywhere. However, image quality is insufficient in
some patients.
Stress Echocardiography
Stress can be used to detect or exclude stenoses of the coronary
arteries and can be performed on a treadmill or a bike. In patients who cannot
exercise, drugs can be used as alternative stressors. A properly performed
stress echocardiogram with a normal result excludes a significant stenosis of a
coronary artery with a high level of confidence. The main limitation of the
test is its dependence on a well trained operator. In some patients, image quality
is not sufficient to perform a stress echocardiogram.
Trans-Oesophageal Echocardiography (TEE)
A TEE can be performed with the same machine as a standard echocardiogram, but it requires a different probe. During this test, the patient is sedated. The small probe, containing an ultrasound transducer at its tip, is placed down the patient’s oesophagus. Being close to the heart, the ultrasound has only a small way to travel.
Structures including both atria, the atrial septum, the left
atrial appendage, the heart valves, and the aorta of the heart can be
visualised with more detailed images than with the standard trans-thoracic echocardiogram.
Heart valve abnormalities can be seen with high image quality. The limitation
of the test is its semi-invasive nature but the risk of the test is very low.
Despite sedation the test may be uncomfortable for some patients. The coronary
arteries cannot be visualised.
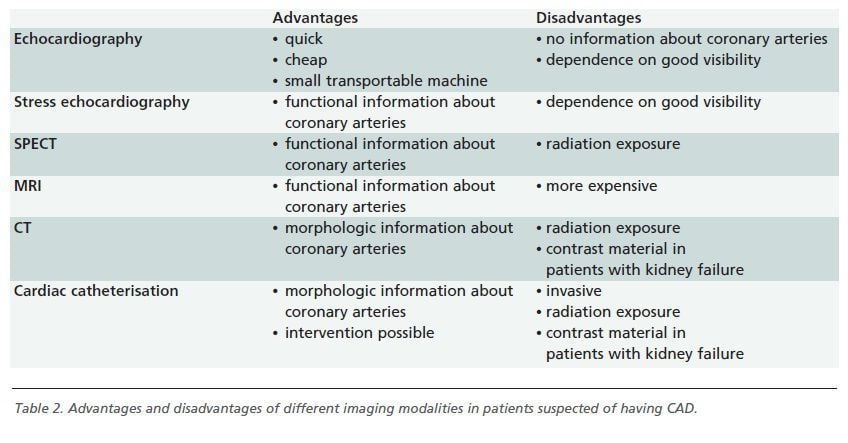
Nuclear Imaging
Stress myocardial perfusion imaging with single-photon computed
tomography (SPECT) uses radioactive tracers to gather information about
regional blood flow, coronary artery perfusion and ventricular function and has
a high diagnostic accuracy in patients with suspected CAD. In patients
incapable of exercise, pharmacologic stress SPECT has comparable accuracy. A
normal perfusion scan is associated with an excellent outcome. With newer radioactive
tracers the size and function of the left ventricle can be measured. The
primary disadvantages are radiation exposure and the expense of the procedure.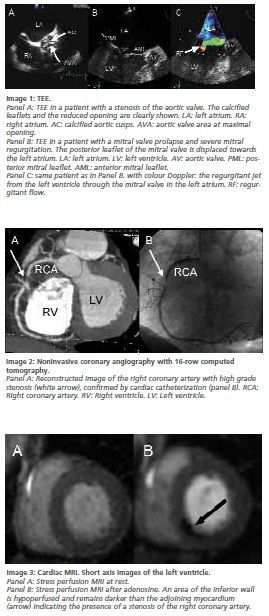
Coronary Angiography and Left Heart Ventriculography
Coronary angiography is an invasive method of visualising the coronary
arteries. In most cases, a catheter is inserted in the groin and pushed to the
heart. The coronary arteries are filled with contrast media so the internal
lumen of the coronary tree can be seen and all stenoses can be demonstrated. The
outer parts of the coronary arteries can’t be seen as only contrast media or
calcified structures appear on the radiographic images. Image resolution of the
coronary tree is higher than with any other method.
If a stenosis or occlusion of a vessel is found, an intervention
can be performed during the same session. In patients with acute myocardial
infarction with elevation of the ST-segments in the ECG, immediate coronary
angiography can save lives. The left ventricle can be filled with contrast
medium and contractions of the left ventricular myocardium demonstrated.
The disadvantages of coronary angiography are radiation, the need for contrast media and its invasiveness.
Magnetic Resonance Imaging
Cardiac MRI is the most accurate technique for evaluating ventricular size and function. It is useful in the evaluation of cardiac masses and congenital heart disease.
Cardiac MRI angiography is a standard technique for imaging the aorta and the large vessels. After administration of gadolinium-containing contrast material, myocardial infarction scars can be detected with a sensitivity unparalleled by any other technique and characteristic patterns of contrast enhancement can be visualised in a variety of myocardial diseases like amyloidosis and hypertrophic cardiomyopathy.
The disadvantages of cardiac MRI are the expense and the need
for contrast material although MR contrast agents are not nephrotoxic. However,
serious side effects were recently described in patients with renal failure.
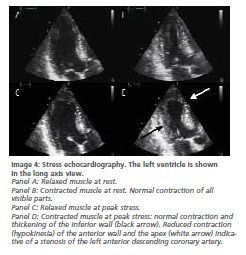
Computed Tomography
With CT of the heart, either coronary calcifications can be measured or a non invasive coronary angiography can be performed. No contrast material is needed. The amount of coronary artery calcium is indicative of the atherosclerotic plaque burden and is associated with the cardiac prognosis. However, the amount of coronary calcium does not correlate with the focal stenosis severity of a given lesion and is therefore unhelpful in predicting the necessity of an intervention.
High resolution non invasive coronary angiography is now feasible. 64-slice multi-detector CT has good sensitivity and a high specificity for the exclusion of high-grade coronary stenoses.
Disadvantages of CT angiography are high radiation exposure and
the need to administer contrast media.
Summary
Echocardiography is the main non invasive imaging method in heart disease. It is quickly performed, relatively cheap and has no side effects. A good echocardiography laboratory is thus mandatory in all cardiology departments.
In patients suspected of having CAD who have an ambiguous stress-test or are not able to exercise stress echocardiography or SPECT myocardial perfusion imaging should be performed. Which technique is performed depends on local expertise and availability. Stress echocardiography has the advantage of not being accompanied by radiation exposure. Expertise in at least one of the techniques should be maintained in all cardiology departments. With coronary angiography, an optimal morphologic diagnosis can be established which may be the basis for an intervention performed in one session.
In the last few years, cardiac MRI and cardiac CT have shown great promise in patients with CAD and other heart diseases. Cardiac MRI has been shown to be very useful in a variety of myocardial diseases. Cardiac CT is able to visualise coronary artery stenoses with high accuracy. However, their role in patients with suspected CAD and other heart diseases has yet to be defined precisely.

