




Anatomical dead space, alveolar dead space, and CO2 elimination: Learn how they can give you an insight into the patient's lung condition.
Single breath CO2 analysis: insight into the patient‘s lung condition
The volumetric capnogram can also be divided into three areas:
- Area X ‑ CO2 elimination
- Area Y ‑ Alveolar dead space
- Area Z ‑ Anatomical dead space
The size of the areas, as well as the form of the curve, can give you more insight into the patient‘s lung condition regarding:
- Dead space fraction ‑ VDaw /VTE
- Alveolar minute ventilation ‑ V‘alv
In the illustration (Figure 1) you can see:
- Slope of Phase III
- Slope of Phase II
- The intersection of lines 1 and 2 defines the limit between Phases II and III
- A perpendicular line is projected onto the X‑axis and its position is adjusted until the areas p and q on both sides become equal
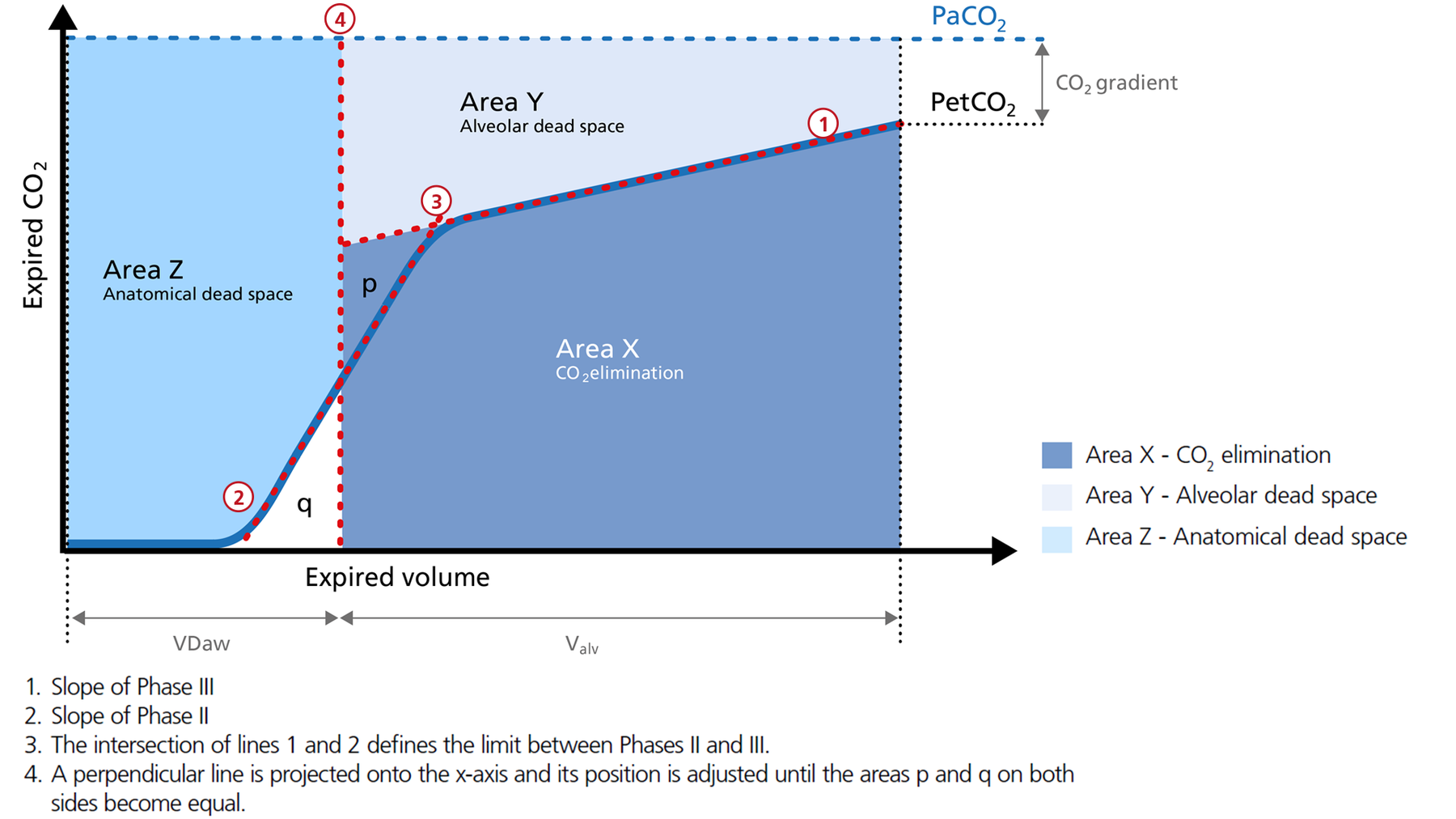
Figure 1: The three areas of the volumetric capnogram
Area X ‑ CO2 elimination (V‘CO2)
Area X represents the actual volume of CO2 exhaled in one breath (VeCO2). Adding up all of the single breaths in one minute gives you the total elimination of CO2 per minute (V‘CO2). If cardiac output, lung perfusion, and ventilation are stable, this is an assessment of the production of CO2 called V‘CO2. The V‘CO2 value displayed on the ventilator can be affected by any change in CO2 production, cardiac output, lung perfusion, and ventilation. It indicates instantly how the patient’s gas exchange responds to a change in ventilator settings. Monitoring trends allows for detection of sudden and rapid changes in V‘CO2 (Figure 2).
Good to know:
Decreasing V‘CO2: Hypothermia, deep sedation, hypothyroidism, paralysis, and brain death decrease CO2 production and induce a decrease in V‘CO2. Decreasing V‘CO2 can also be due to a decrease in cardiac output or blood loss, and may also suggest a change in blood flow to the lung areas. Pulmonary embolism, for example, exhibits V‘CO2 reduction and a slope reduction in Phase II.
Increase in V‘CO2: An increase in V'CO2 is usually due to bicarbonate infusion or an increase in CO2 production that can be caused by:
- Fever
- Sepsis
- Seizures
- Hyperthyroidism
- Insulin therapy
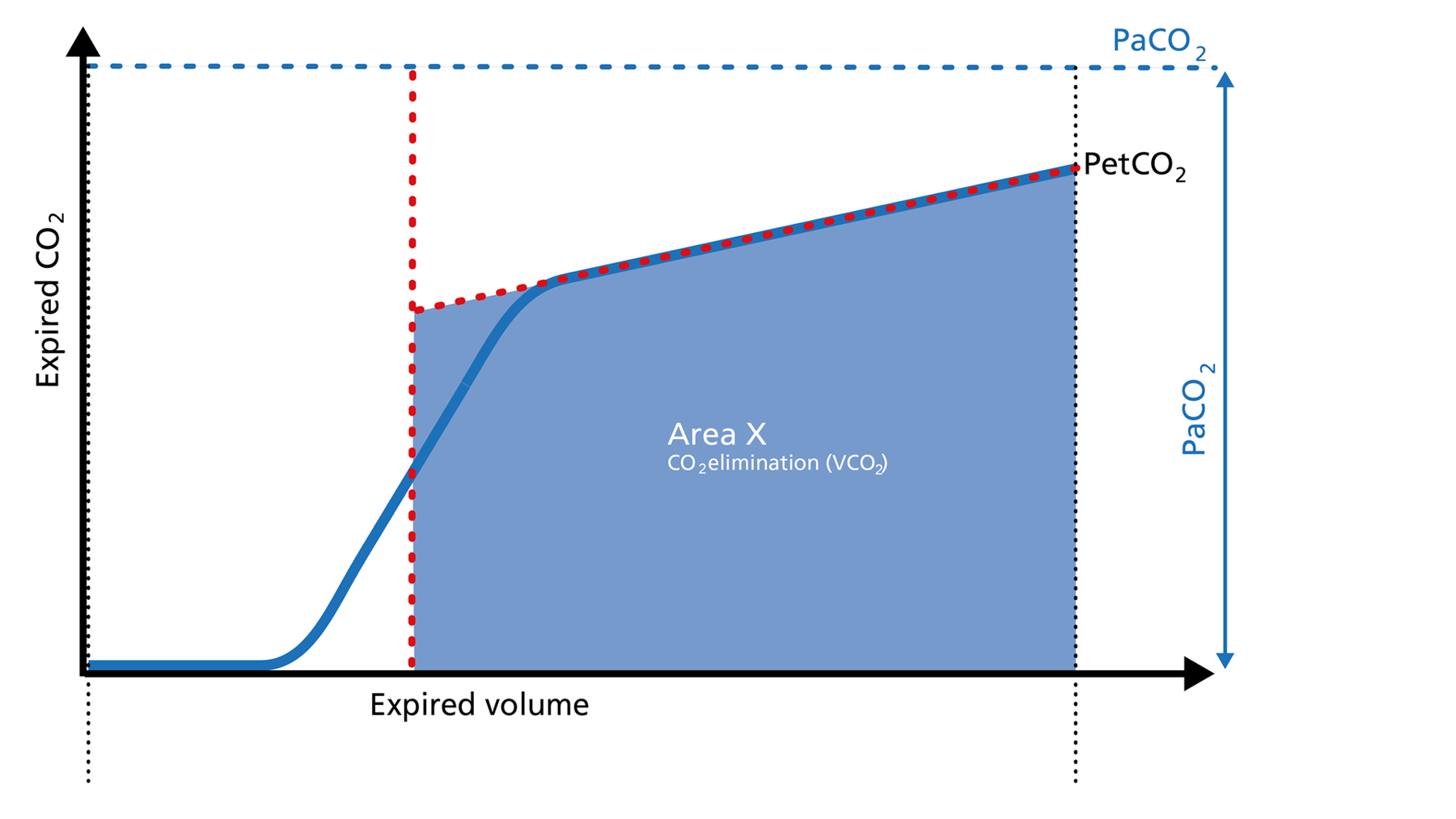
Figure 2: Area X of the volumetric capnogram
Area Y ‑ Alveolar dead space
Area Y represents the amount of CO2 that is not eliminated due to alveolar dead space (Figure 3).
Good to know:
Increase: Alveolar dead space is increased in cases of lung emphysema, lung overdistension, pulmonary embolism, pulmonary hypertension, and cardiac output compromise.
Decrease: If the above mentioned conditions improve due to successful therapy, the alveolar dead space decreases.
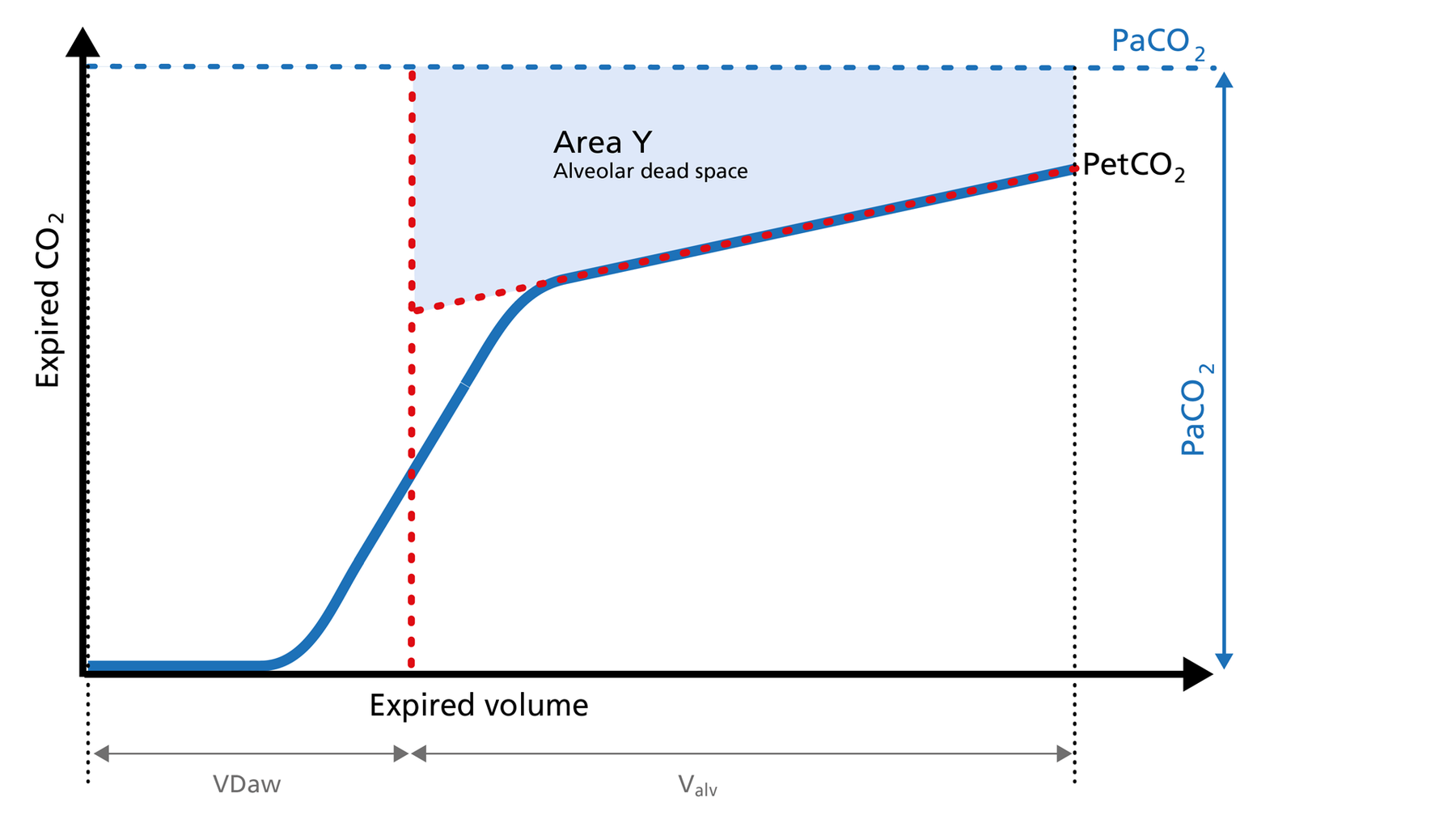
Figure 3: Area Y of the volumetric capnogram
Area Z ‑ Anatomical dead space
Anatomical dead space measurement using a volumetric capnogram gives an effective, in‑vivo measure of volume lost in the conducting airway. This area represents a volume without CO2. It does not take part in the gas exchange and consists of the airway, endotracheal tube, and artificial accessories, such as a flextube positioned between the CO2 sensor and the patient (Figure 4).
Good to know:
Expansion of Area Z: An expansion of Area Z can indicate an increase in anatomical dead space ventilation (VDaw). Consider a reduction in your artificial dead space volume.
Diminution of Area Z: A diminution of Area Z is seen when the artificial dead space volume is decreased and when excessive PEEP is decreased.
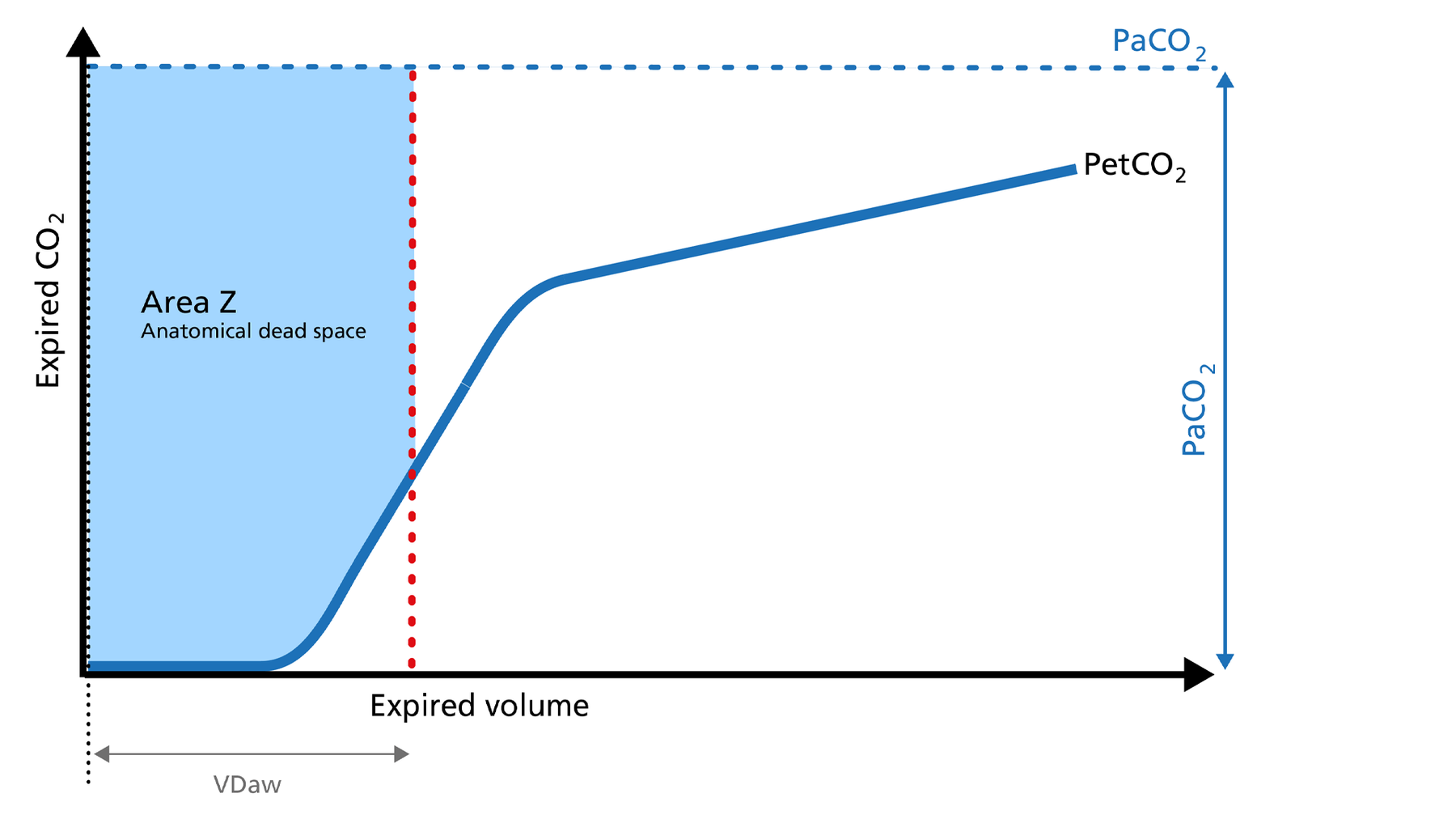
Figure 4: Area Z of the volumetric capnogram
Alveolar minute ventilation ‑ V‘alv
Phase III of the waveform represents the quantity of gas that comes from the alveoli and actively participates in gas exchange. V‘alv is calculated by subtracting the anatomical dead space (VDaw) from the tidal volume (VTE) multiplied by the respiratory rate from the minute volume (MinVol): V’alv =RR*Vtalv = RR*(VTE‑VDaw) (Figure 5).
Good to know:
Increase: An increase in V‘alv is seen after an efficient recruitment maneuver and induces a transient increase in V‘CO2.
Decrease: A decrease in V‘alv can indicate that fewer alveoli are participating in the gas exchange, for example, due to pulmonary edema.
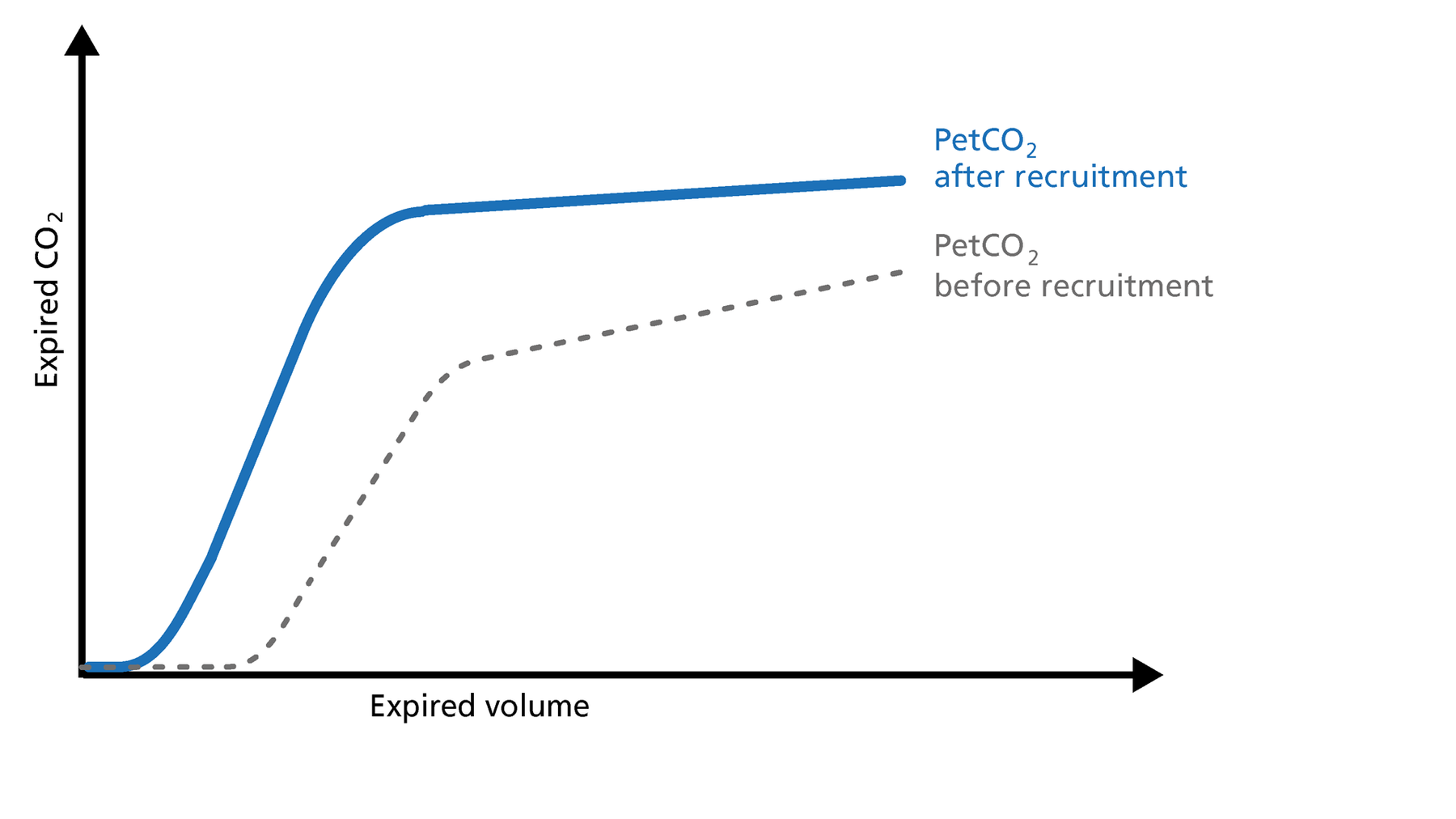
Figure 5: PetCO2 before and after recruitment
Dead space ventilation ‑ VDaw/VTE ratio
The ratio of airway dead space (VDaw) to tidal volume (VTE) ‑ the VDaw/VTE ratio ‑ gives you an insight into the effectiveness of ventilation (Figure 6).
Good to know: A rising VDaw/VTE ratio can be a sign of ARDS.
- In a normal lung, the VDaw/VTE ratio is between 25% and 30%.
- In early ARDS, it is between 58% and up to 83%.
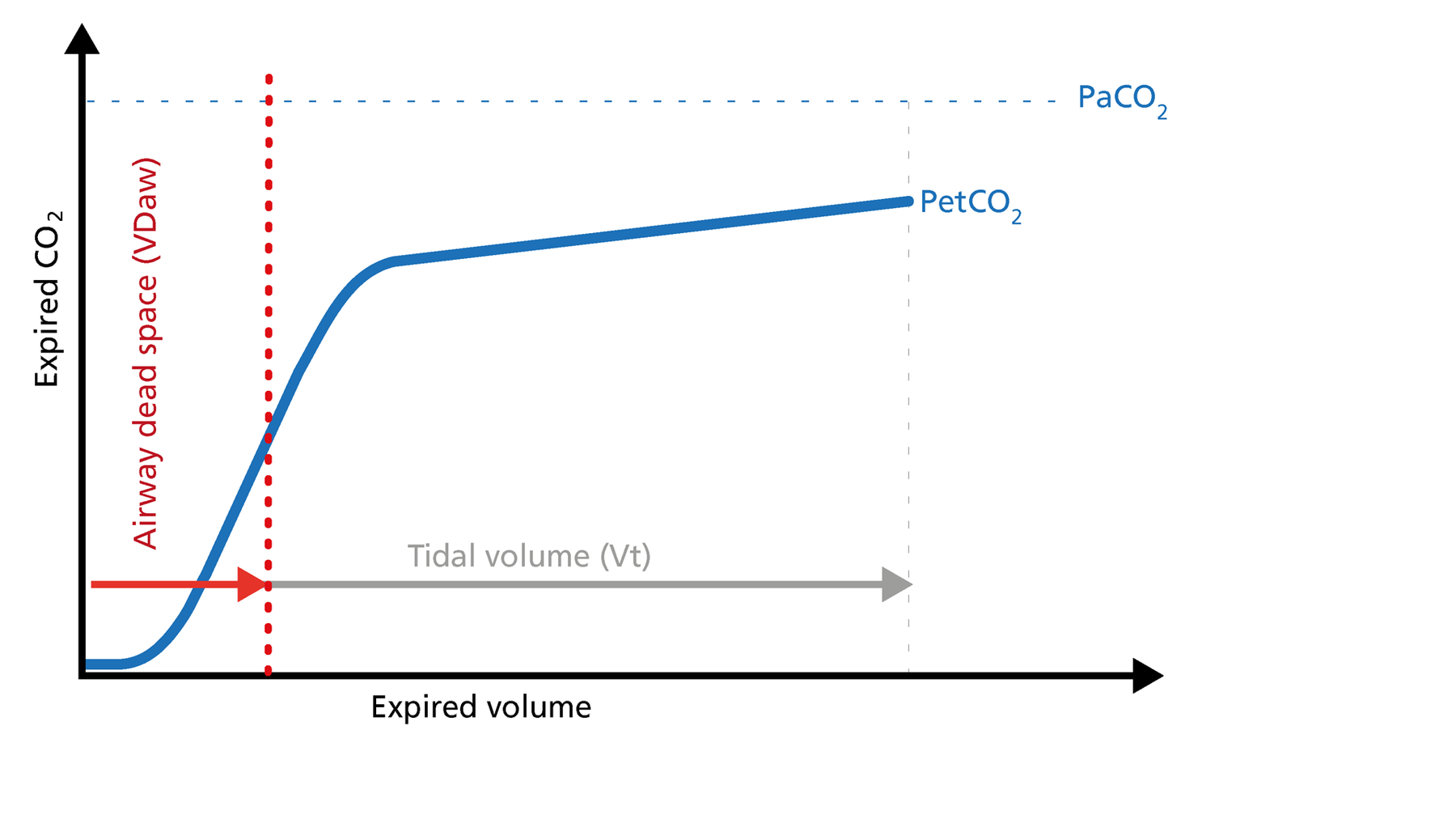
Figure 6: Dead space ventilation
Volumetric capnography on Hamilton Medical ventilators
All Hamilton Medical ventilators offer volumetric capnography (All models except HAMILTON‑MR1A). It is available as an option on the HAMILTON‑C6, the HAMILTON‑G5, the HAMILTON‑C3, and the HAMILTON‑C1/T1, and as a standard feature on the HAMILTON‑S1.
Author: Karjaghli Munir, Respiratory Therapist, Hamilton Medical Clinical Application Specialist; Matthias Himmelstoss, ICU Nurse, MSc Physics, Product Manager
Date of first publication: 16.11.2023
Source: Hamilton Medical
References:
- Anderson JT, Owings JT, Goodnight JE. Bedside noninvasive detection of acute pulmonary embolism in critically ill surgical patients. Arch Surg. 1999;134(8):869‑875. doi:10.1001/archsurg.134.8.869
- Aström E, Niklason L, Drefeldt B, Bajc M, Jonson B. Partitioning of dead space‑‑a method and reference values in the awake human. Eur Respir J. 2000;16(4):659‑664. doi:10.1034/j.1399‑3003.2000.16d16.x
- Blanch L, Romero PV, Lucangelo U. Volumetric capnography in the mechanically ventilated patient. Minerva Anestesiol. 2006;72(6):577‑585.
- Eriksson L, Wollmer P, Olsson CG, et al. Diagnosis of pulmonary embolism based upon alveolar dead space analysis. Chest. 1989;96(2):357‑362. doi:10.1378/chest.96.2.357
- Fletcher R, Jonson B, Cumming G, Brew J. The concept of deadspace with special reference to the single breath test for carbon dioxide. Br J Anaesth. 1981;53(1):77‑88. doi:10.1093/bja/53.1.77
- Kallet RH, Daniel BM, Garcia O, Matthay MA. Accuracy of physiologic dead space measurements in patients with acute respiratory distress syndrome using volumetric capnography: comparison with the metabolic monitor method. Respir Care. 2005;50(4):462‑467.
- Kiiski R, Takala J. Hypermetabolism and efficiency of CO2 removal in acute respiratory failure. Chest. 1994;105(4):1198‑1203. doi:10.1378/chest.105.4.1198
- Kumar AY, Bhavani‑Shankar K, Moseley HS, Delph Y. Inspiratory valve malfunction in a circle system: pitfalls in capnography. Can J Anaesth. 1992;39(9):997‑999. doi:10.1007/BF03008353
- Nuckton TJ, Alonso JA, Kallet RH, et al. Pulmonary dead‑space fraction as a risk factor for death in the acute respiratory distress syndrome. N Engl J Med. 2002;346(17):1281‑1286. doi:10.1056/NEJMoa012835
- Eriksson L, Wollmer P, Olsson CG, et al. Diagnosis of pulmonary embolism based upon alveolar dead space analysis. Chest. 1989;96(2):357‑362. doi:10.1378/chest.96.2.357
- Pyles ST, Berman LS, Modell JH. Expiratory valve dysfunction in a semiclosed circle anesthesia circuit‑‑verification by analysis of carbon dioxide waveform. Anesth Analg. 1984;63(5):536‑537.
- RADFORD EP Jr. Ventilation standards for use in artificial respiration. J Appl Physiol. 1955;7(4):451‑460. doi:10.1152/jappl.1955.7.4.451
- Rodger MA, Jones G, Rasuli P, et al. Steady‑state end‑tidal alveolar dead space fraction and D‑dimer: bedside tests to exclude pulmonary embolism. Chest. 2001;120(1):115‑119. doi:10.1378/chest.120.1.115
- Yaron M, Padyk P, Hutsinpiller M, Cairns CB. Utility of the expiratory capnogram in the assessment of bronchospasm. Ann Emerg Med. 1996;28(4):403‑407. doi:10.1016/s0196‑0644(96)70005‑7
- Wolff G, Brunner JX, Grädel E. Gas exchange during mechanical ventilation and spontaneous breathing. Intermittent mandatory ventilation after open heart surgery. Chest. 1986;90(1):11‑17. doi:10.1378/chest.90.1.11
- Wolff G, X. B. J. , Weibel W., Bowes C.L. , Muchenberger R., Bertschmann W. (1989). Anatomical and series dead space volume: concept and measurement in clinical practice. Applied cardiopulmonary pathophysiology, 2, 299‑307.
















