



HealthManagement, Volume 3 - Issue 1, 2009
Since 1978, the Italian healthcare system has been organised according to the National Health Service model (Italian National Health Service, or INHS). Coverage is universal and, theoretically, uniform throughout the country. In 2003, public healthcare expenditure accounted for 75.1% of total healthcare expenditure. The Italian healthcare system is tax-funded and most care is provided free of charge at the point of service.
How is Care Provided?
Care is provided by government entities - Local Health Units (LHUs) and Independent NHS hospitals as well as private hospitals and professionals that are eligible for reimbursement when “accredited” by the relevant Region. The INHS has three tiers: the central government at the top; 21 regional governments in between; and 180 LHUs and 95 IHs at the bottom.
INHS staff (including about 660,000 people, 1.1% of the Italian
population) are under national contracts; wages and salaries are based on
position and age. General practitioners (about 55,000) are not INHS employees,
but provide primary care and refer patients to higher levels of care. From 1978
to 1992, the INHS was characterised by centralised funding based on past
expenditures.
Reforms Include “New” Managerialism
In the 1990s, the INHS underwent a major reform introducing managerialism, de centralisation to regions and quasi-markets. Under managerialism, many hospitals were taken out of LHU control and established as independent entities (IHs); general managers replaced highly politicised boards of trustees; LHUs and IHs were given greater decision-making autonomy, but were also required to meet higher performance standards.
Under decentralisation, regional governments achieved greater control over LHUs and IHs, appointed their general managers, provided them with guidelines, and is expected to cover the deficits. Under this new arrangement, each region became a parent company with LHUs and IHs as its subsidiaries. So much so, that some claim Italy no longer has one National Health Service but rather 21 regional ones. At present, a further decentralisation process is under discussion, giving more power to regions on health and requiring that funding be collected at regional level, with an interregional equalisation fund to guarantee national equity on per capita funding.
Quasi-market mechanisms were expected to induce better performance
by requiring money to “follow patients”. As a general rule, each LHU will
reimburse other LHUs, IHs and accredited private providers for care given to
its residents. Reimbursements are DRG based for hospital discharges and
fee-for-service for outpatient services. Under this general framework, each
region is free to design its own funding arrangements. Italy’s regions have
consequently been experimenting with different organisational and funding
models to achieve an acceptable combination of equity, efficiency, freedom of
choice and cost containment.
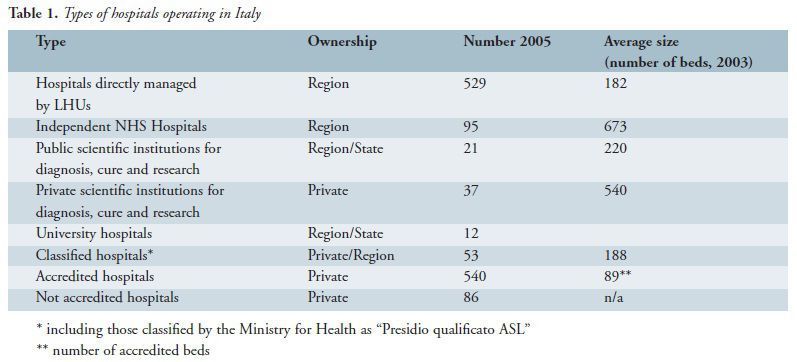
The Italian Hospital System
Hospitals have always played a central role in the INHS. Table 1 shows the different types of hospitals operating in Italy in terms of number, ownership and size.
In the last few years, health policy has pursued a shift from
hospital to ambulatory care, resulting in a sharp decrease in the number of
public hospitals (from 1,068 in 1995 to 732 in 2003) and public acute beds
(from about 300,000 in 1995 to 200,000 in 2003). In contrast, accredited
hospitals have remained stable (about 530 hospitals and 50,000 beds), probably
because they focused on rehabilitation, long-stay and chronic disease care
traditionally. The current density of NHS beds is 4.8 for 1000 inhabitants (4.2
beds for acute care and 0.6 for non-acute care).
Internal Organisation
The head of each public healthcare organisation (LHUs and IHs) is a General Manager (GM) appointed by the region. He is accountable for his performance and could be dismissed, if deemed inadequate. The replacement of highly politicised Boards of Trustees with a GM was one of the most significant INHS reforms in the 1990s, marking a sharp departure from the traditional bureaucratic paradigm.
This spoil system showed some strengths but also weaknesses. In particular, regions were replacing their GMs too frequently. Nationwide, the average GM tenure was 3.2 years between 1996 and 2003. This seemed too short a period for effective management, especially in view of the complexity of healthcare organisations; the marked discontinuities brought about by GM turnover in the absence of strong managerial systems and market discipline; and the destabilising effects of turnover expectations.
Traditionally, the organisational structure of public hospitals was fragmented into numerous small, independent departments (e.g. general medicine, nephrology, gastroenterology). Numerous publications had recommended that these departments merge into larger “divisions” or “clinical directorates” to reach an effective compromise between specialisation and integration, and create a team of clinical managers interfacing the professionals with the GM. Managerialism reforms encouraged public providers to follow this recommendation.
According to a survey in 2003, clinical directorates had been
introduced by 92% of public providers and extended to all inpatient medical and
surgical units by 77%. Despite the introduction of clinical directorates, the
most important level of responsibility centres still corresponded to the
traditional, fragmented departments.
Financing
As mentioned, the reforms of the 1990s significantly changed the funding system for public and accredited providers, from the traditional model based on past expenditures to a model where LHUs were financed on an adjusted capitation basis and money followed patients when they chose to receive care not from their own LHU of residence but from IHs, accredited private providers or other LHUs.
The purpose is to place healthcare organisations under further pressure to improve efficiency and quality of care and reduce waiting lists. The undesirable effect may lead to an excessive increase in the volume of services provided to LHU residents by other LHUs, IHs and private providers, where “excessive” means “unnecessary”.
Consequently, all the regions try to limit this potential distortion by means of:
- Differentiated fee
schedules (according to the private or public nature of healthcare organisations
and to their organisational complexity and case-mix);
- Lump sum funding for activities where DRG based or fee for service
funding is deemed unfeasible or inappropriate (e.g. funding emergency
departments);
- Expenditure ceilings and targets defined by the region for each
single provider or negotiation of bilateral contracts between LHUs and
providers; and
- Introduction of utilisation reviews to deny payment for services that do not meet specified appropriateness criteria and development of appropriateness guidelines especially for out-patient services.













