




An entirely new and novel approach in targeting the brain in stroke rehabilitation therapy was presented today at the annual meeting of the Radiological Society of North America (RSNA). With stroke affecting millions of people worldwide, rehabilitation still has room for improvement. Only 5% of stroke patients make a full recovery, and current therapies do not use the patient's brain to rebuild lost neural pathways and do not closely link intent to move with activation of afflicted limbs. Using a novel stroke rehabilitation device that converts an individual's thoughts to electrical impulses to move upper extremities, stroke patients in this study reported improvements in their motor function and ability to perform activities of daily living.
Vivek Prabhakaran, MD, Ph.D., director of functional neuroimaging in radiology at the University of Wisconsin-Madison., along with co-principal investigator Justin Williams, Ph.D., and a multidisciplinary team, built the new rehabilitation device - brain computer interface technology, by pairing a functional electrical stimulation (FES) system, which is currently used to help stroke patients recover limb function, and a brain control interface (BCI), which provides a direct communication pathway between the brain and this peripheral stimulation device.
In an FES system, electrical currents are used to activate nerves in paralysed extremities. Using a computer and an electrode cap placed on the head (pictured), the new BCI-FES device (called the Closed-Loop Neural Activity-Triggered Stroke Rehabilitation Device) interprets electrical impulses from the brain and transmits the information to the FES.
"FES is a passive technique in that the electrical impulses move the patients' extremities for them," Dr. Prabhakaran said. "When a patient using our device is asked to imagine or attempt to move his or her hand, the BCI translates that brain activity to a signal that triggers the FES. Our system adds an active component to the rehabilitation by linking brain activity to the peripheral stimulation device, which gives the patients direct control over their movement." He aded that one of its key advantages is that the patient controls the therapy, and it can be used irrespective of motor function.
The Wisconsin team conducted a small clinical trial of their rehabilitation device with eight patients with one hand affected by stroke. The patients were also able to serve as a control group by using their normal, unaffected hand. Patients in the study represented a wide range of stroke severity and amount of time elapsed since the stroke occurred, up to 2 years. Despite having received standard rehabilitative care, the patients had varying degrees of residual motor deficits in their upper extremities. Each underwent nine to 15 rehabilitation sessions of two to three hours with the new device over a period of three to six weeks.
The patients also underwent functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI) before, at the mid-point of, at the end of, and one month following the rehabilitation period. fMRI is able to show which areas of the brain are activated while the patient performs a task, and DTI reveals the integrity of fibres within the white matter that connects the brain's functional areas.
Patients who suffered a stroke of moderate severity realised the greatest improvements to motor function following the rehabilitation sessions. Patients diagnosed with mild and severe strokes reported improved ability to complete activities of daily living following rehabilitation.
Dr. Prabhakaran said the results captured throughout the rehabilitation process—specifically the ratio of hemispheric involvement of motor areas—related well to the behavioral changes observed in patients. A comparison of pre-rehabilitation and post-rehabilitation fMRI results revealed reorganisation in the regions of the brain responsible for motor function. DTI results over the course of the rehabilitation period revealed a gradual strengthening of the integrity of the fibre tracts.
"Our hope is that this device not only shortens rehabilitation time for stroke patients, but also that it brings a higher level of recovery than is achievable with the current standard of care," Dr. Prabhakaran said. "We believe brain imaging will be helpful in both planning and tracking a stroke patient's therapy, as well as learning more about neuroplastic changes during recovery."
Potentially the system could be very cost-effective by allowing the patient to continue rehabilitation in the home setting. The system's technology could be made available as a portable end product where the EEG cap, FES system and the PC/laptop are integrated and controlled by a table size system, at a cost of US$500-1500.
Dr. Prabhakaran and his team are continuing to work on the system by training patients in a short session in the laboratory followed by home setup to allow use over a longer period.
Other co-authors are Dorothy Farrar-Edwards, Ph.D., Justin Sattin, MD, Mitch Tyler, Ph.D., Veena A. Nair, Ph.D., Svyatoslav Vergun, B.S., Leo Walton, B.S., Jie Song, M.S., and Brittany Young, B.A., B.S.
Images
Main image shows a stroke patient receiving therapy using the BCI-FES device.
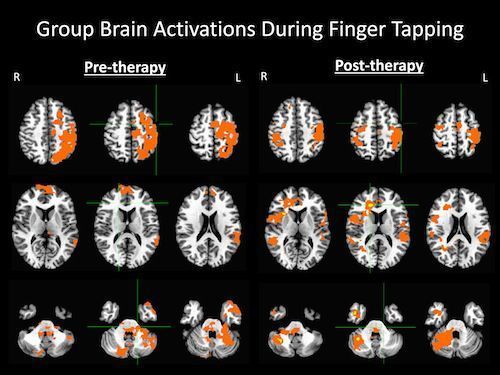
Figure 1. Brain activation patterns produced as patients tapped the fingers of their impaired hand before and after four to six weeks of therapy using the BCI-FES device.
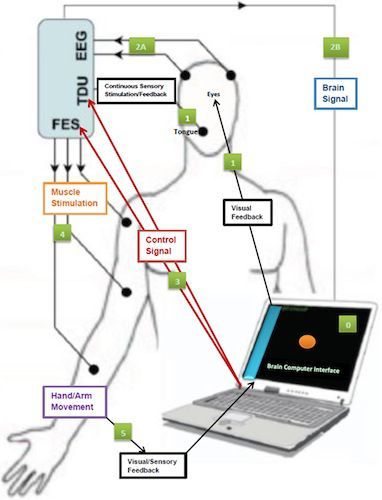
Figure 2. A schematic representation of the BCI-FES device indicating input and feedback components.
Latest Articles
Stroke, rehabilitation, functional MRI
An entirely new and novel approach in targeting the brain in stroke rehabilitation therapy was presented today at the annual meeting of the Radiological So...




















