




When TIME magazine called PET-CT imaging the invention of the year in 2000, the value of hybrid imaging was recognised by the public as well as doctors. But who should perform these studies? Gerald Antoch, Professor of Radiology and Chair of the Radiology department at the University of Düsseldorf in Germany, addressed this topic at the European Congress of Radiology in Vienna this week, as presenter of the Wilhelm Conrad Röntgen honorary lecture.
If you believe the vendors, said Antoch, then a good hybrid imaging system is all that is needed for conclusive diagnosis. However, to quote Einstein:
“Computers are incredibly fast, accurate, and stupid. Human beings are incredibly slow, inaccurate, and brilliant. Together they are powerful beyond imagination. But a good imaging system is nothing more than a good or big computer."
You still need the personnel to define the protocols and read the images. So how did the experts view the dilemma in the early days of hybrid imaging?
But, to quote Churchill, “An expert is a person who later can say exactly why his forecast didn’t meet!”
With the advent of hybrid imaging, hospitals have had to tackle firstly the issue of image acquisition, namely who is the responsible department (radiology or nuclear medicine), who provides the technicians and are both modalities wanted to be diagnostic. Who reports, and should there be one or two reports? Who liaises with referring physicians and markets the service? Lastly, there is the issue of reimbursement.
Antoch admitted he is fortunate to be in an academic hospital where a dual service can operate. In his institution two technicians acquire the images, then either a NM or radiology resident reports, and both a board-certified radiologist and a board-certified nuclear physician approve the report before it is uploaded to the PACS. Citing Fischman and Thrall (2010) there are three potential workflows for reading and interpreting PET-CT studies. University hospitals can offer subspecialised reading. Larger hospitals depend on a close relationship between the two disciplines, while in private practice and community-based hospitals it is more practical to have one person trained in the dual disciplines. In the real world, acknowledge Antoch, the workflow needs to address limited resources and be cost-effective, so have a technicians trained in both disciplines and reporting by a doctor who is dual trained.
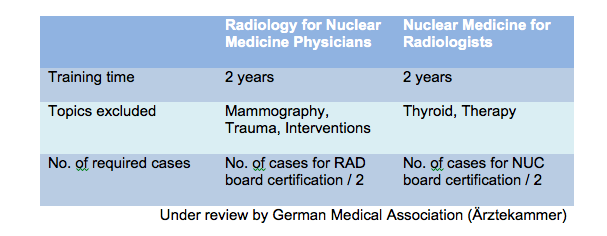
While training is dependent on local and country-specific regulations, there is the possibility of hybrid training. For doctors, this can include being board-certified in both disciplines or an additional qualification in the other specialty after board certification, all with a common trunk of training in imaging. This was addressed by an article by Coleman et al. in J Nucl Med. In the U.S. the ACR has neither approved nor endorsed the training requirements proposed in this document for the interpretation of diagnostic CT scans. In Germany the German Medical Association is reviewing the proposal for training for both disciplines.
The ESR and European Association of Nuclear Medicine published their white paper in 2007 on multimodality imaging, stating that “It is therefore important that the two specialities review their relationship to maximise the success of the technical advances for our patients, and to avoid a damaging confrontation which would be negative for the profession, for the future of both specialities and for the public that we serve.”
For the future the training could encompass a common trunk of imaging for two years, followed by specialisation in radiology, nuclear medicine or hybrid imaging, each for a period of three years.
Antoch’s vision is for one imaging centre, with a flat structure, so that section chiefs have equal rights. Linking reiumbursement to the imaging centre rather than to the individual departments may help to solve the turf battle problem. Let’s not have a turf battle, he said.
To create a real hybrid, bringing together two modalities together is not enough. What is needed is specialists for conclusive and accurate diagnosis, new training concepts, and integrating both disciplines into one Imaging Department.
In closing, Antoch quoted the carmaker Daimler, who said “The worldwide demand for automobiles will not exceed 1 million - only because of a lack of available chauffeurs!”
Let the two worlds of radiology and nuclear medicine come together - we need to provide enough chauffeurs rather than have none or let others provide them, concluded Antoch.
Claire Pillar
Managing Editor, HealthManagement.org
If you believe the vendors, said Antoch, then a good hybrid imaging system is all that is needed for conclusive diagnosis. However, to quote Einstein:
“Computers are incredibly fast, accurate, and stupid. Human beings are incredibly slow, inaccurate, and brilliant. Together they are powerful beyond imagination. But a good imaging system is nothing more than a good or big computer."
You still need the personnel to define the protocols and read the images. So how did the experts view the dilemma in the early days of hybrid imaging?
- “CT is nothing more but anatomical correlation and attenuation correction of PET” (nuclear medicine expert)
- “FDG is nothing more but the new contrast agent for CT” (radiology expert)
But, to quote Churchill, “An expert is a person who later can say exactly why his forecast didn’t meet!”
With the advent of hybrid imaging, hospitals have had to tackle firstly the issue of image acquisition, namely who is the responsible department (radiology or nuclear medicine), who provides the technicians and are both modalities wanted to be diagnostic. Who reports, and should there be one or two reports? Who liaises with referring physicians and markets the service? Lastly, there is the issue of reimbursement.
Antoch admitted he is fortunate to be in an academic hospital where a dual service can operate. In his institution two technicians acquire the images, then either a NM or radiology resident reports, and both a board-certified radiologist and a board-certified nuclear physician approve the report before it is uploaded to the PACS. Citing Fischman and Thrall (2010) there are three potential workflows for reading and interpreting PET-CT studies. University hospitals can offer subspecialised reading. Larger hospitals depend on a close relationship between the two disciplines, while in private practice and community-based hospitals it is more practical to have one person trained in the dual disciplines. In the real world, acknowledge Antoch, the workflow needs to address limited resources and be cost-effective, so have a technicians trained in both disciplines and reporting by a doctor who is dual trained.
While training is dependent on local and country-specific regulations, there is the possibility of hybrid training. For doctors, this can include being board-certified in both disciplines or an additional qualification in the other specialty after board certification, all with a common trunk of training in imaging. This was addressed by an article by Coleman et al. in J Nucl Med. In the U.S. the ACR has neither approved nor endorsed the training requirements proposed in this document for the interpretation of diagnostic CT scans. In Germany the German Medical Association is reviewing the proposal for training for both disciplines.
The ESR and European Association of Nuclear Medicine published their white paper in 2007 on multimodality imaging, stating that “It is therefore important that the two specialities review their relationship to maximise the success of the technical advances for our patients, and to avoid a damaging confrontation which would be negative for the profession, for the future of both specialities and for the public that we serve.”
For the future the training could encompass a common trunk of imaging for two years, followed by specialisation in radiology, nuclear medicine or hybrid imaging, each for a period of three years.
Antoch’s vision is for one imaging centre, with a flat structure, so that section chiefs have equal rights. Linking reiumbursement to the imaging centre rather than to the individual departments may help to solve the turf battle problem. Let’s not have a turf battle, he said.
To create a real hybrid, bringing together two modalities together is not enough. What is needed is specialists for conclusive and accurate diagnosis, new training concepts, and integrating both disciplines into one Imaging Department.
In closing, Antoch quoted the carmaker Daimler, who said “The worldwide demand for automobiles will not exceed 1 million - only because of a lack of available chauffeurs!”
Let the two worlds of radiology and nuclear medicine come together - we need to provide enough chauffeurs rather than have none or let others provide them, concluded Antoch.
Claire Pillar
Managing Editor, HealthManagement.org
Latest Articles
When TIME magazine called PET-CT imaging the invention of the year in 2000, the value of hybrid imaging was recognised by the public as well as doctors. Bu...
















