




INTRODUCTION
A study of emergency admissions in England found that over a quarter of admissions did not require an overnight stay (length of stay [LoS] of zero).1 This suggests that many emergency patients could benefit from ambulatory emergency care (AEC).1
Fundamental to AEC is the identification and management of patients with acute medical conditions that do not require overnight admission.2 This entails immediate access to urgent care that would usually require the resources and expertise available in an acute hospital.3
BACKGROUND
Effective AEC can deliver streamlined, efficient patient care within one working day.4 This may improve clinical outcomes, the patient experience, and costs.4,5 The Royal College of Physicians (RCP) speculates that, in the near future, emerging technologies, such as improved with-patient point of care testing (POCT) platforms, are likely to offer more options for managing patients in an AEC setting.4 Integrated POCT devices, such as the i-STAT System™, could be a key part of the future of AEC.
The James Paget University Hospital (JPUH) cares for approximately 240,000 residents across Great Yarmouth, Lowestoft and Waveney, as well as visitors coming to East Anglia.6,7 The number of yearly emergency admissions at the JPUH is approximately 67,000.7
Within the JPUH Acute Medicine Unit (AMU), the Emergency Assessment and Discharge Unit (EADU) was used for the immediate review and treatment of patients who were expected to require inpatient therapies and investigations, while the AEC unit served less dependent patients.8
As the AEC service was unable to meet demand, steps were taken to redesign the patient management streams and form a new unit called the Ambulatory Care Unit (AmbU).9
This culminated in a “proof-of-concept” pilot, using POCT and process change, which were in line with NHS best practice guidelines and RCP principles.1,10,11 With no central laboratory service at the AEC site, the use of with-patient POCT, using devices such as the i-STAT System, was seen as a key method in improving efficiency.12 The pilot was later extended with financing from the Trust and approved as a business case to provide a permanent service.11 This white paper discusses both the process and results of the AEC redesign at JPUH.
THE JPUH AEC REDESIGN
PROCESS
Project team
The project team included hospital staff, who collaborated with multidisciplinary stakeholders and industry partners. Industry partner support/sponsorship was obtained from Abbott Point-of-Care, Radiometer® and Operasee Limited.7,11,12
Systematic approach to process redesign
The AEC redesign process consisted of evidence-based methodologies, including:7,12
• Demand and Process Activity Mapping to understand how the current system worked and to identify an evidence-based, ideal future-state, capable of fulfilling demand. This identified leverage points on which to focus, such as POCT, to catalyse change
• Failure Mode Effect Analysis (FMEA), which is a step-by-step approach to identifying all possible failures in a design, process, product or service. FMEA was utilised to provide evolving process governance, and to obtain input from multiple stakeholders to identify, quantify, prioritise and resolve potential issues in terms of severity, occurrence and detection
RESULTS
Reduced patient LoS was identified as the goal of the redesigned AEC service and POCT as a method of leveraging change (Figure 1)12
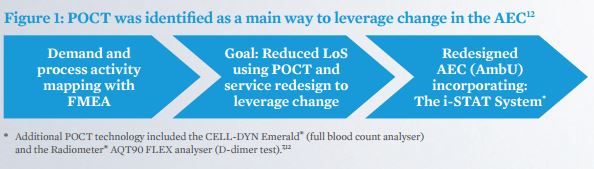
To reach the goal of reduced LoS, the new service implemented the following:
• POCT, including the i-STAT System
• Appropriate treatment/discharge planning
• Early senior clinical decision maker input
• Condition-specific management algorithms (outlined by the RCP3) POCT fulfilled over 85% of patient diagnostic needs in the AEC setting.7
The i-STAT System, in particular, was used for a variety of common tests, with the following cartridges used most widely:7*
• CHEM8+ to test blood electrolytes, basic haematology parameters and TCO2
• CG4+ to test lactate and blood gases
• PT/INR to test prothrombin time (a measure of blood coagulation) Additionally, the CELL-DYN Emerald® analyser performed full blood count testing and the Radiometer® AQT90 FLEX carried out D-dimer tests.7,12
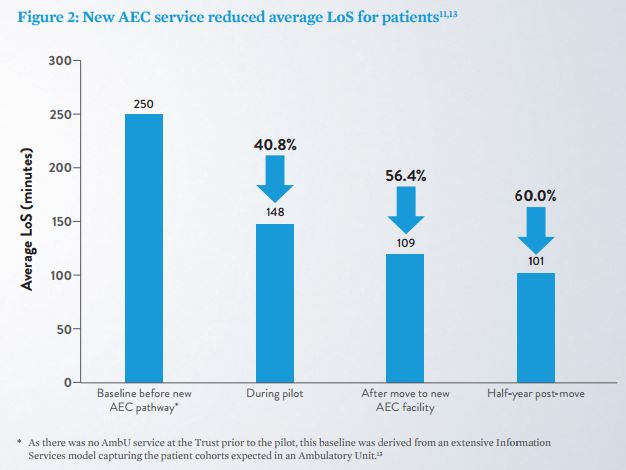
New AEC service demonstrated dramatic improvements in LoS The new AEC pathway started in August 2014 (Monday through Friday, 08:30–18:30). It began as a three-month pilot, which led to dramatic improvements in patient flow and reductions in LoS (Figure 2). These improvements continued post-pilot and after the AmbU moved into a newly-built environment (within the AMU) with additional staff to support the extended service (Figure 2).11,13
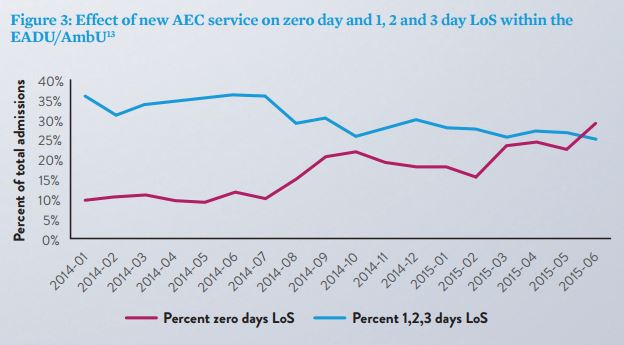
New AEC service improved zero day LoS rate within EADU/AmbU admissions Emergency care was expedited as a result of the new outpatient AEC service, in both the EADU and the AmbU. The rate of patients going home on the same day increased and the rate of patients admitted for 1, 2 or 3 days decreased, demonstrating that fewer patients required overnight stays. The reduced LoS was achieved despite the patient admission rate remaining constant (Figure 3).13
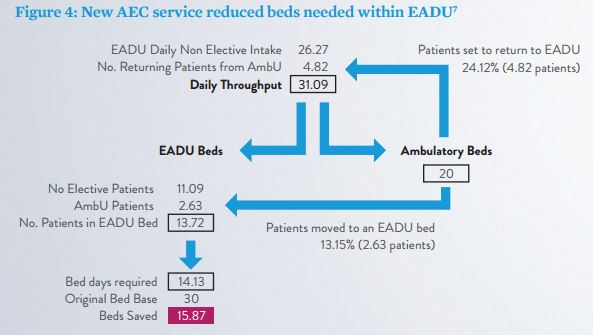
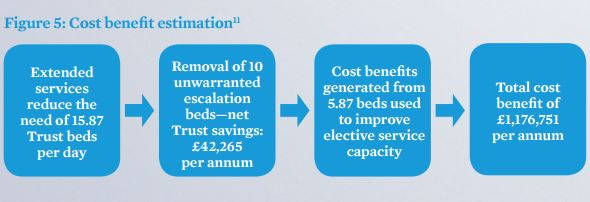
New AEC service has a proposed economic benefit of more than £1 million Following the pilot’s success, a business case was approved to provide 7-day AEC services, with operational hours extended from 08:30–18:30 to 08:00–21:30.11 It was calculated that the extended AEC services would save 15.87 Trust beds per day within the EADU (Figure 4).7
Despite the decrease in overnight stays, reducing Trust income (representing a £557,146 saving for the Clinical Commissioning Group), and the cost of providing the service (increased staffing and POCT diagnostics, etc.), it was estimated that implementation of the service would result in a net Trust saving of £42,265 per annum in the acute setting— through the safe removal of 10 unwarranted escalation beds. The remaining capacity (approximately 5.87 beds) could be used to improve elective service capacity. This equates to a total economic cost benefit of £1,176,751 per annum (Figure 5). 11
DISCUSSION
The new AEC service at JPUH concentrated on the implementation of POCT and process redesign.11 Integrated POCT devices, such as the i-STAT System (providing multiple traditionally laboratory-associated tests on a portable single platform), are designed to provide rapid diagnostic information that enables faster clinical management decisions. Within the new AEC service, this helped reduce LoS and costs.11 Other benefits may also be realised when POCT is incorporated into a workflow that allows real-time availability of results, including improved patient satisfaction and clinical outcomes.5
Additional POCT benefits experienced at this site included:
• Patient data integration within the hospital information system7, 14
• Senior clinical decision maker review within one hour 12
• Static readmission rates12
• Positive patient feedback with 79% “extremely likely” to recommend the service12
• Under 10 minutes to initial review 12
In the hospital setting, inefficient triage systems, prolonged radiology and central laboratory turnaround times, along with insufficient/non-flexible staffing, contribute to inefficient operations and patient queuing.15 By incorporating process redesign changes, the AmbU has become an integral part of the emergency care system within the JPUH.8
Following the pilot, some staff felt that the i-STAT System gave them more time with the patient. They also felt that it increased their ability to communicate with the patients about their results.
Conclusion
The overall changes to process and adoption of the ambulatory model, along with integration of POCT, such as the i-STAT System, and evidence-based service redesign, have achieved reduced LoS for medical patients simultaneously with a proposed economic benefit of more than £1 million.11
Source & Image Credit: Abbott
References
- NHS Institute for Innovation and
Improvement. Ambulatory care directory for adult patients. 2009.
- McCallum L et al. National
ambulatory care survey: current level of adoption and considerations for the
future. Clin Med 2010;10(6):555–9.
- Royal College of Physicians. Acute
Medical Care – the right person, in the right setting – first time. Report of
the Acute Medicine Task Force 2007. London. Available at: www.rcplondon.ac.uk/sites/default/files/documents/acute_medical_care_final_for_web.pdf
[Accessed July 2016].
- Royal College of Physicians. Acute
care toolkit 10 Ambulatory emergency care. October 2014. Available at: https://www.rcplondon.ac.uk/guidelines-policy/acute-care-toolkit-10-ambulatory-emergency-care
[Accessed July 2016].
- St John A. The Evidence to Support
Point-of-Care Testing. Clin Biochem Rev 2010;31:111–9.
- JPUH website. About us. Available
at: http://www.jpaget.nhs.uk/about-us/ [Accessed July 2016].
- Weihser P. Utilising POCT and
Service Redesign to Establish an Ambulatory Emergency Care Service. James Paget
University Hospitals – NHS. September 8, 2015. [Unpublished presentation].
- JPUH website. Acute Medicine.
Available at: http://www.jpaget.nhs.uk/departments-services/departments-services-a-z/acute-medicine/
[Accessed July 2016].
- Giles D et al. Establishing an
acute ambulatory care service. The Clinical Services Journal. April 2015.
Available at http://www.clinicalservicesjournal.com/story/14275/establishing-an-acute-ambulatory-care-service
[Accessed July 2016 - login needed].
- NHS England. 2015/16 National
Tariff Payment System: A consultation notice – Annex 4a: Additional information
on currencies with national prices. November 26, 2014. Available at:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/379571/S118_Annex_4A_NTCN1516.pdf
[Accessed July 2016].
- Giles D et al. Health Services
Journal ‘Acute Sector Innovation Award’ Application – Executive Summary. 2015.[Unpublished
Document].
- Giles D et al. Attaining a 90
Minute Length of Stay – Ambulatory Care Redesigned. James Paget University
Hospitals –NHS. Poster presented at the Society for Acute Medicine (SAM)
Manchester 10-11 September 2015. Available at: http://www.acutemedicine.org.uk/wp-content/uploads/2015/10/SOD-7-Attaining-a-90-minute-length-of-stay-Ambulatory-Emergency-Care-Redesigned.pdf[Accessed July 2016].
- Data on file. Abbott POC.
- Conworx. Device Interface List
POCcelerator™. Available at: http://www.conworx.com/en/produkte/item/download/518_e86656b2305e47e5ec84c74202f41cc8
[Accessed July 2016].
- Seay T and Fite DL. Approaching
Full Capacity in the Emergency Department. American College of Emergency
Physicians.October 2006. Available at:
http://www.acep.org/workarea/DownloadAsset.aspx?id=8852 [Accessed July 2016].
















