





A study of over 1 million ICU patients has found that just 5 percent of patients account for 33 percent of ICU bed days. And the researchers, led by Theodore Iwashyna, MD, Associate Professor of Internal Medicine at the University of Michigan (U-M) Health System and a member of the VA Center for Clinical Management Research and the U-M Institute for Healthcare Policy and Innovation, have identified these patients as having the condition of persistent critical illness or PerCI. Iwashyna and his co-researchers hope that the findings lead to research into better care and treatment to prevent patients from becoming persistently critically ill, and to discover which hospitals are successful at lifting patients out of PerCI and treating those patients who do succumb to PerCI.
The team, which also included researchers from the VA Ann Arbor Healthcare System in the U.S. and Monash University in Melbourne, Australia, based their work on data from more than 1 million ICU patients held by the Australian and New Zealand Intensive Care Society Centre for Outcome and Resource Evaluation Registries (ANZICS CORE). The 1,028,235 critically ill patients were treated in 182 ICUs across Australia and New Zealand between 2000 and 2014. The study findings are due to be published in Lancet Respiratory Medicine. In an email to ICU Management & Practice, senior author, Professor Rinaldo Bellomo, from Monash University, explained that this is the first study to have devised a logical, valid and reproducible approach to identify persistently critically ill patients and to have tested it in >1 million ICU patients.
The researchers looked at the patients’ hospital records to see how well each patient’s eventual outcome could be predicted, using the standard severity of illness scores and also new risk scores developed by Monash University statistician Michael Bailey, PhD. These risk scores included the specific diagnosis that led to hospital admission and also specific in-hospital test results and monitoring of vital signs and physiology. The researchers also looked at whether a patient's risk of dying could be predicted by factors that related to his or her pre-hospital state, including age, gender and pre-existing chronic conditions. They found that after about 10 days in the ICU, the usual clinically-based prediction tools lost their power to predict risk of death. Who the patient was before he or she came to the hospital mattered more to their chance of dying. This point signals transition to PerCI, say the researchers. The transition occurred some time during the 2nd week in the ICU, although it could be sooner or later, depending on the diagnosis.
Dr. Iwashyna confirmed that PerCI is a separate state that patients transition into: “you're there because you're there, stuck in this cascade that we can't get you out of," he said. He added: "The reason why these patients came in to the hospital in the first place doesn't matter nearly as much anymore - what matters is that they've been there, and some aspects of how well their body worked before they came in, such as age. These [patients] are the ones where no matter how hard we try, we can't get them balanced. You feel like you should be able to get ahead of the things that keep erupting in them. You're always chasing yesterday's problem, and meanwhile they're developing tomorrow's problem," from pneumonia and gastrointestinal bleeding to sepsis and Clostridium difficile infections.
Prof. Bellomo commented that better understanding of PerCI could assist ICU teams in discussing prospects for patients who have been in the ICU a long time. "We need to help the fraction who are inevitably going to die do so with dignity, and at the same time help those who are not fated to die to get better treatment," he said. He explained that the knowledge from this study will be helpful to target this unique high risk group of patients for preventive intervention and for specific interventions to accelerate recovery and improve outcomes - “Defining such patients opens the door to understanding why they developed PerCI”. He added that the research team hope to replicate this study with the U.S. Veterans Administration database in the next 12 months.
In addition to Iwashyna, Bellomo, and Hodgson, the research team included David Pilcher, MD, Michael Bailey, PhD, Allison van Lint, PhD and Shaila Chavan, MS of Monash.
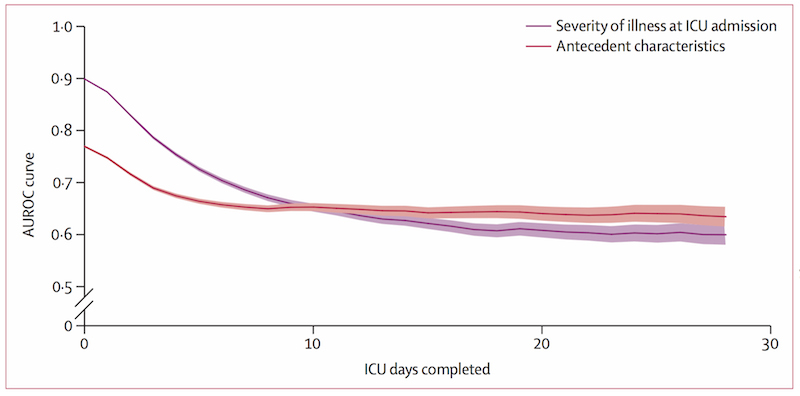
Around Day 10 of an ICU stay, patients enter a state called persistent critical illness, or PerCI, where the reason they entered the hospital becomes less important than who they were before they became ill or injured. The graph is based on data from more than a million ICU patients treated in Australia and New Zealand. Image credit: University of Michigan and Monash University.
Source: University of Michigan Health System
The team, which also included researchers from the VA Ann Arbor Healthcare System in the U.S. and Monash University in Melbourne, Australia, based their work on data from more than 1 million ICU patients held by the Australian and New Zealand Intensive Care Society Centre for Outcome and Resource Evaluation Registries (ANZICS CORE). The 1,028,235 critically ill patients were treated in 182 ICUs across Australia and New Zealand between 2000 and 2014. The study findings are due to be published in Lancet Respiratory Medicine. In an email to ICU Management & Practice, senior author, Professor Rinaldo Bellomo, from Monash University, explained that this is the first study to have devised a logical, valid and reproducible approach to identify persistently critically ill patients and to have tested it in >1 million ICU patients.
Findings
Of the million patients included in the study, 51,509 were found to have what the researchers define as PerCI. The PerCI patients spent more than a million days in ICU beds, and more than 2.2 million days in the hospital overall. Nearly one-quarter of the patients with PerCI died in the ICU. Just under half were able to go directly home from the hospital - compared with three-quarters of non-PerCI ICU patients.The researchers looked at the patients’ hospital records to see how well each patient’s eventual outcome could be predicted, using the standard severity of illness scores and also new risk scores developed by Monash University statistician Michael Bailey, PhD. These risk scores included the specific diagnosis that led to hospital admission and also specific in-hospital test results and monitoring of vital signs and physiology. The researchers also looked at whether a patient's risk of dying could be predicted by factors that related to his or her pre-hospital state, including age, gender and pre-existing chronic conditions. They found that after about 10 days in the ICU, the usual clinically-based prediction tools lost their power to predict risk of death. Who the patient was before he or she came to the hospital mattered more to their chance of dying. This point signals transition to PerCI, say the researchers. The transition occurred some time during the 2nd week in the ICU, although it could be sooner or later, depending on the diagnosis.
Dr. Iwashyna confirmed that PerCI is a separate state that patients transition into: “you're there because you're there, stuck in this cascade that we can't get you out of," he said. He added: "The reason why these patients came in to the hospital in the first place doesn't matter nearly as much anymore - what matters is that they've been there, and some aspects of how well their body worked before they came in, such as age. These [patients] are the ones where no matter how hard we try, we can't get them balanced. You feel like you should be able to get ahead of the things that keep erupting in them. You're always chasing yesterday's problem, and meanwhile they're developing tomorrow's problem," from pneumonia and gastrointestinal bleeding to sepsis and Clostridium difficile infections.
Next Steps
Carol Hodgson, PhD, a Monash University ICU physiotherapist and second author, explained that PerCI focuses on different characteristics of patients than other efforts used to describe long-stay patients, such as ‘failure-to-wean’. "That label focuses the care team on the particular details of respiratory mechanics," she said. "Our clinical experience and our data suggest instead that the problem may be that PerCI patients may never even reach the point where ICU doctors are able to try to get them off a ventilator - they just keep cascading from new problem to new problem. These patients need particular strategies that may prevent or reduce PerCI within the ICU, and additional resources to facilitate safe discharge from the ICU and hospital, with only 50% able to be discharged home."Prof. Bellomo commented that better understanding of PerCI could assist ICU teams in discussing prospects for patients who have been in the ICU a long time. "We need to help the fraction who are inevitably going to die do so with dignity, and at the same time help those who are not fated to die to get better treatment," he said. He explained that the knowledge from this study will be helpful to target this unique high risk group of patients for preventive intervention and for specific interventions to accelerate recovery and improve outcomes - “Defining such patients opens the door to understanding why they developed PerCI”. He added that the research team hope to replicate this study with the U.S. Veterans Administration database in the next 12 months.
In addition to Iwashyna, Bellomo, and Hodgson, the research team included David Pilcher, MD, Michael Bailey, PhD, Allison van Lint, PhD and Shaila Chavan, MS of Monash.
Around Day 10 of an ICU stay, patients enter a state called persistent critical illness, or PerCI, where the reason they entered the hospital becomes less important than who they were before they became ill or injured. The graph is based on data from more than a million ICU patients treated in Australia and New Zealand. Image credit: University of Michigan and Monash University.
Source: University of Michigan Health System
References:
Theodore J Iwashyna TJ, Hodgson CL, Pilcher D, Bailey M, van Lint A Chavan S, Bellomo R (2016) Timing of onset and burden of persistent critical illness in Australia and New Zealand: a retrospective, population-based, observational study. Lancet Respir Med, published online May 4, http://dx.doi.org/10.1016/S2213-2600%2816%2930098-4.
Iwashyna TJ, Hodgson CL, Pilcher D, Orford N, Santamaria JD, Bailey M, Bellomo R (2015) Towards defining persistent critical illness and other varieties of chronic critical illness. Crit Care Resusc, 17(3):215-8.
Iwashyna TJ, Hodgson CL, Pilcher D, Bailey M, Bellomo R (2015) Persistent critical illness characterised by Australian and New Zealand ICU clinicians. Crit Care Resusc, 17(3): 153-8.
Iwashyna TJ, Hodgson CL, Pilcher D, Orford N, Santamaria JD, Bailey M, Bellomo R (2015) Towards defining persistent critical illness and other varieties of chronic critical illness. Crit Care Resusc, 17(3):215-8.
Iwashyna TJ, Hodgson CL, Pilcher D, Bailey M, Bellomo R (2015) Persistent critical illness characterised by Australian and New Zealand ICU clinicians. Crit Care Resusc, 17(3): 153-8.
Latest Articles
critically ill, persistent critical illness, PerCI
A study of over 1 million ICU patients has found that just 5 percent of patients account for 33 percent of ICU bed days. And the researchers, led by Theodore Iwashyna, MD, Associate Professor of Internal medicine at the University of Michigan (U-M) Health
















