



HealthManagement, Volume 1 - Issue 1, November-December 2007
Cardiovascular disease (CVD) is responsible for half of all deaths in Europe every year and 25% of chronic disease burden. Aside from the direct effects on human health and welfare CVD costs the European economy over €169 billion per year. The scale of the problem in human and fiscal terms means that urgent action is required to reduce the CVD burden in the population.
Who is at Risk?
At one end of the spectrum are those young individuals who need healthy lifestyle advice to shift their CVD risk downwards. In this group relatively modest intervention is necessary to have a major effect in decades to come. At the other end of the spectrum, for those people with established CVD, current therapies are in place to attempt to reduce and delay the likelihood of recurrent events, although their residual risk still remains very high.
In the middle are the
largest group, who are at moderate risk but have not yet manifest CVD.
Assessing risk in these individuals is complex. Since the risk factors for CVD
are highly prevalent in the population they are poor discriminators of whether
an individual will develop CVD (see fig. 1). Also, there is considerable variability
in an individual’s susceptibility to risk factors.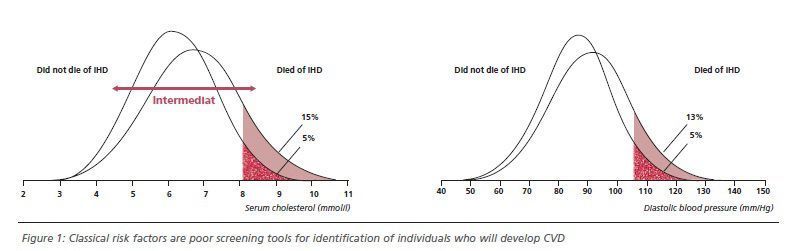
Need for Improved Risk Assessment Factors
Risk assessment tools (e.g. Framingham score) are widely available and are excellent at predicting risk in populations but far less useful for the individual where risk factor susceptibility is also important. There is need for improved and personalised risk assessment. Recently, two noninvasive techniques, carotid intima-media thickness (IMT) measurement and pulse wave velocity (PWV), have emerged as potential tools to refine risk assessment for CVD in individuals.
Carotid IMT measures the thickness of the intima media layer in the carotid artery using high resolution ultrasound; PWV uses Doppler ultrasound or photoplethysmography to determine the speed of transit of the pulse wave through large conduit arteries. Rather than simply measuring the presence or severity of classical risk factors these techniques determine the consequences of the risk factors directly in the blood vessels where atherosclerosis occurs.
Carotid IMT and PWV
increase with age in normal individuals and by relating the results of these
tests to large population data bases, it is possible to simplify the results as
a measure of the vascular age in years. A simple comparison of the chronological
and vascular age immediately allows the individual an assessment of the state
of their arteries. Our experience has suggested that patients find the interpretation
of risk difficult, whereas they readily understand if their arteries are ten
years older than their chronological age. These techniques measure the consequences
of the risk factors, therefore they may provide information on individual susceptibility.
Carotid IMT Technology
Carotid ultrasound is usually used to determine the presence of carotid stenosis in people who have had a cerebrovascular event or in asymptomatic people found to have a carotid bruit. Using high frequency B-mode ultrasound systems resolution is high enough to see the individual layers of the carotid artery wall and to measure the intima-media thickness. The key advance in this assessment has come from the development of accurate image analysis that allows measurement using automatic computer software.
IMT can be easily and
reliably used to determine vascular age. Some investigators are now using the
IMT estimated vascular age as a substitute for chronological age to recalculate
Framingham risk. In one study 50% of people at moderately high risk (10-20%)
had a significant change in risk classification with 28% increasing and 22%
decreasing. These changes are important because they can be translated into
alteration in the intensity of drug therapy.
Integrating Carotid IMT
into Risk Assessment
Carotid IMT can be integrated with standard cardiovascular risk assessment in a one-stop vascular clinic run by a cardiologist or physician and supported by a vascular technologist. In our clinic, using a portable ultrasound system measurements take about twenty minutes to perform and the analysis is completed immediately using on board computer software.
The only potential
disadvantage to performing carotid IMT measurement routinely is the requirement
for relatively expensive equipment (~30,000 Euro), a trained individual to
perform data acquisition and analysis and the addition of time to the clinical
assessment. For these reasons other technologies which are cheaper and operator
independent deserve further consideration. One such technology is the
measurement of vascular stiffness.
Pulse Wave Analysis Technology
Identifying premature vascular stiffening is of value in the detection of cardiovascular disease. Arterial stiffness can be determined indirectly by velocity of the pressure pulse as it travels through the arterial system. Pulse wave velocity is measured using Doppler ultrasound to detect the arrival of the pulse at the carotid and femoral arteries and timing this against the onset of ventricular systole on the electrocardiogram.
Pulse wave velocity is a strong independent predictor of CVD risk in patients with end stage renal disease, hypertension, the elderly and diabetics and has been shown to predict CVD events better than Framingham risk equations. An increase in pulse wave velocity of one standard deviation above the mean is associated with a 39% increase in risk independent of classical CVD risk factors.
Pulse wave analysis can be time consuming, though newer technology analyses the shape of the digital volume pulse (DVP) obtained from an infra-red sensor using a technique called photo-plethysmography. The stiffer the arteries the quicker the pulse waves travel and therefore the smaller is this delay. By dividing the subject’s height in metres by the time delay between the direct and reflected waves it is possible to determine a stiffness index. Stiffness index and pulse wave velocity are closely correlated with <4% difference when compared directly.
In the age of personalised medicine, both Carotid IMT and Pulse Wave analysis are likely to have increased uptake and become established as a routine part of cardiovascular screening and risk assessment.

