

 vs Surgery")

 vs Surgery")
Late-breaking research presented at ESC Congress 2024 revealed no significant difference in efficacy between transcatheter edge-to-edge repair (TEER) and surgery for patients with secondary mitral regurgitation (MR).
TEER is a common treatment for secondary MR, but until now, no randomised trial has compared it with surgery. The MATTERHORN trial showed that both techniques are equally effective in improving MR, with TEER offering some safety advantages.
The investigator-initiated, randomised controlled MATTERHORN trial enrolled patients with secondary MR, left ventricular ejection fraction (LVEF) ≥20%, heart failure symptoms (NYHA class ≥2) despite optimal medical therapy, and high surgical risk as assessed by the local Heart Team. Participants were randomised 1:1 to receive either mitral TEER or surgical mitral valve therapy.
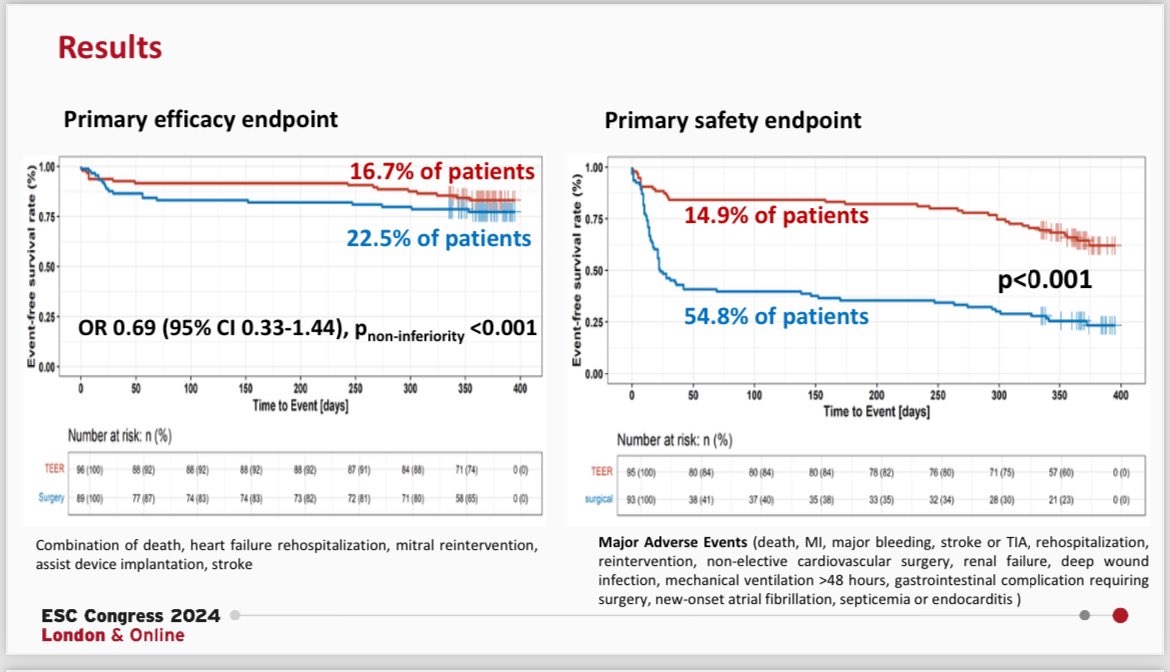
The primary efficacy endpoint was a composite of death, hospitalisation for heart failure, mitral reintervention, assist device implantation, and stroke at one year. The key secondary endpoint was MR grade ≥3 recurrence at one year. The primary safety endpoint, assessed at 30 days, included death, myocardial infarction, major bleeding, stroke or transient ischaemic attack, rehospitalisation, all reinterventions, non-elective cardiovascular surgery, renal failure, deep wound infection, mechanical ventilation >48 hours, gastrointestinal complications requiring surgery, new-onset atrial fibrillation (AF), sepsis, and endocarditis.
A total of 210 patients were randomised across 16 centres in Germany. The average age was 70.5 years, 40% were female, and the mean LVEF was 43%. Most patients (86%) had NYHA class III or IV heart failure, and the median EuroSCORE II was 3%. In the surgical group, 72% underwent mitral valve repair, while 28% had mitral valve replacement.
Results showed no significant difference in the primary composite endpoint, which occurred in 16.7% of the TEER group and 22.5% of the surgical group at one year, confirming non-inferiority. There was also no significant difference in MR recurrence (grade ≥3) at 1 year: 8.9% in the TEER group versus 1.5% in the surgical group. At 1 year, 73.2% of TEER patients and 87.3% of surgical patients had MR grade ≤1, demonstrating the efficacy of both treatments.
However, the primary safety endpoint occurred significantly more often in the surgical group (54.8%) compared to the TEER group (14.9%), driven mainly by higher rates of major bleeding (29% vs. 3%), all reinterventions (19% vs. 8%), and new-onset AF (33% vs. 9%).
The MATTERHORN trial is the first randomised trial to demonstrate the non-inferiority of TEER and surgery in patients with secondary MR. These findings could influence decision-making as current European guidelines suggest TEER may be considered for patients deemed inoperable or at high surgical risk.
Source, Slides and Image Credit: ESC Congress 2024